다발경화증의 인지 장애와 평가
Cognitive Dysfunction and Assessment in Multiple Sclerosis
Article information
Trans Abstract
Cognitive impairment is a common and disabling feature of multiple sclerosis (MS), affecting up to 65% of patients. It primarily manifests as deficits in processing speed, memory, executive function, and verbal fluency, significantly influencing daily activities and work performance. Despite its clinical relevance, cognitive assessment in MS remains underutilized. Several neuropsychological tools, including the multiple sclerosis neuropsychological questionnaire, the symbol digit modalities test, and the brief international cognitive assessment for MS, facilitate early detection of cognitive impairment. Moreover, depression, anxiety, and fatigue often worsen cognitive decline. Recent research has identified distinct cognitive phenotypes in MS, aiding in personalized management strategies. Integrating cognitive assessments with neuroimaging biomarkers and cognitive rehabilitation is essential for improving patient outcomes. Future studies should focus on refining diagnostic tools and exploring targeted interventions to better support MS patients.
서론
다발경화증(multiple sclerosis, MS)은 중추신경계(central nerve system)를 침범하는 대표적인 자가면역질환(autoimmune disease) 중에 하나로 초기에 탈수초화(demyelinating), 염증 및 축삭(axon)의 손상 등의 증상을 보인다. 또한 MS로 진단받은 사람은 초기 단계부터 인지 기능 장애가 발생할 수 있고 이는 질병 전반에 걸쳐 최대 65%에서 관찰되었다.1 인지 기능 장애는 기억력, 주의 집중력, 언어 능력, 시공간 능력 및 판단력을 포함한 전두엽의 집행 기능 등이 저하된 상태를 의미하며 장애 수준은 단기적이거나 시간이 지남에 따라 악화되거나 또는 영구적일 수 있다. 인지 기능 장애는 전반적인 삶의 질을 저하시키고 이와 함께 우울 및 불안과 같은 정신질환이 함께 동반하기 쉽고 신체적 그리고 정신적 건강을 저해하는 주요한 요인이다.
MS 환자들의 대표적인 인지 저하 영역은 정보처리속도(information processing speed), 일화 기억(episodic memory), 집행 기능(executive function), 언어 유창성(verbal fluency), 시공간 처리(visuospatial processing)로 알려져 있다.2 MS 환자들의 인지 저하의 특징은 환자마다(inter-individual) 다른 증상과 질병 진행 양상을 보이며 매우 이질적인 것으로 알려져 있다. MS 환자들에게서의 인지 저하는 magnetic resonance imaging (MRI) 결과에서 백질병변(white matter lesions)과 뇌 위축(brain atrophy)만으로는 설명이 불충분하며 인지 예비능(cognitive reserve)과 같은 다양한 비구조적 요인에 의해 많은 영향을 받는 것으로 보인다.3 MS 환자들에게서 인지 저하가 더 심각한 형태로 나타나는 경우는 MRI 결과에서 이상 병변의 부피(lesion volume)와 수(lesion count)가 많고 인지 기능과 관련된 특정 뇌 영역인 경우와 더불어 낮은 인지 예비능이 동반될 때이다. MS 환자들을 대상으로 한 반복적인 인지 훈련이 인지 기능 향상을 이끌어낸다는 결과로 미루어 볼 때 기저 인지 장애의 평가를 통한 치료 및 재활의 효과를 확인하기 위해 MS 진단 초기부터 인지 기능에 대한 평가가 필수적이다. MS 환자의 뇌 손상이 적을수록 인지 중재의 결과가 더 좋아지는 것으로 나타났기 때문에,4 가장 효과적인 인지 중재를 확인하기 위해서는 초기부터 인지 장애에 대한 평가가 중요하다. 국제적으로도 MS 환자들의 인지 기능 평가 및 모니터링을 연간 추적조사 방식으로 권장하고 있다.5 그러나 MS 관련 연구들은 주로 운동 장애, 보행 장애, 시력 장애, 감각증상 등에 관한 것이 대다수이기 때문에 인지 기능의 변화를 면밀히 평가하기 위해서는 평가 과정에서 많은 비용과 시간과 소요되고 질환에 특화된 신경 심리 검사 전문가가 필요하기 때문에 임상 현장에서의 적용에서는 어려움이 있다. 인지 장애를 평가하는 도구가 주로 노년기에서 발병률이 높은 알츠하이머 치매, 혈관성 치매 및 파킨슨병과 같은 퇴행성 질환에 동반된 치매에 초점을 맞추고 있는 반면, 비교적 젊은 연령층부터 발병하는 MS 환자들의 특성에 적합한 인지 장애에 적합한 평가 도구를 사용하여 발명 초기부터 장기적인 추적 검사를 통해 MS 환자들의 고유한 인지 장애 특성을 확인하는 것이 중요하다. 이러한 의미에서 국내 외에서 다발경화증에서 주로 사용되는 인지 기능 사용되는 선별 검사와 종합 검사들의 항목들의 비교를 통해 국내 다발경화증에서 인지 장애 평가를 이해하고 임상 현장에서 적절한 검사 방법의 활용에 대해 고찰하고자 한다.
본론
선별 평가(screening test)
스크리닝 검사는 비교적 간단하고 짧은 시간 내에 실시할 수 있으며 민감도와 특이도가 높으며 인지 기능 저하를 조기에 발견할 수 있는 장점이 있으나 이러한 검사는 전문적인 해석이 필요하며 개인의 상황과 병력을 고려하여 종합적인 판단이 이루어져야 한다. 기존 연구에서 MS 환자에게 적용되었던 선별 검사 도구는 다음과 같다(Table 1).
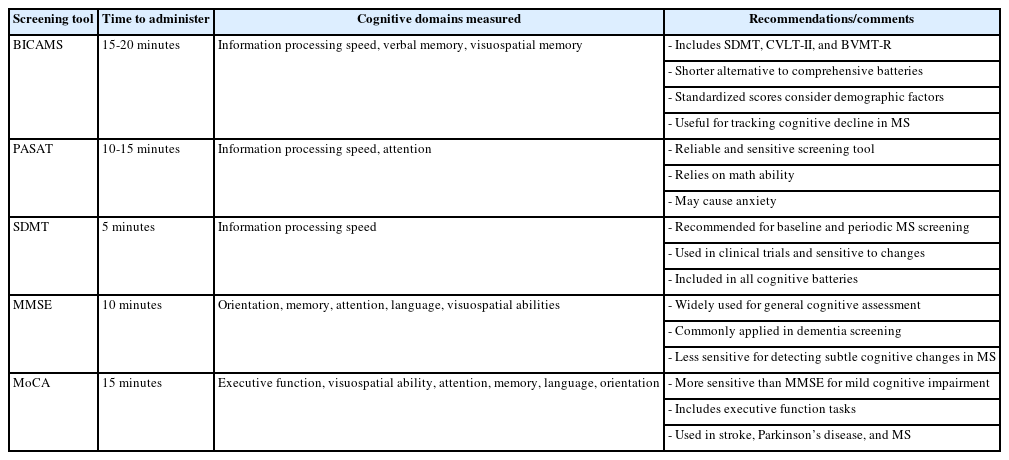
Cognitive screening tools in multiple sclerosis
Multiple sclerosis neuropsychological questionnaire (MSNQ): 다발경화증 신경 심리 설문지
MSNQ는 15개의 항목으로 구성된 설문지로 환자의 주관적인 인지 기능 저하를 파악하는 데 주로 사용된다. 비록 객관적인 인지 평가 도구들과는 구별되지만 임상에서는 인지 기능 저하의 선별 도구로 활용되고 있다. 설문지 하위 항목은 기억력(예: 약속을 잊는다), 주의 집중력(예: 쉽게 주의가 산만해진다), 처리 속도(예: 문제 해결 속도가 느려졌다) 등의 다양한 인지 영역을 평가하며 일상생활에서 역량을 함께 평가한다.6,7 각 문항은 5점 리커트 척도로 각각의 항목에서 ‘매우 그렇다(4점)’, ‘대체로 그렇다(3점)’, ‘보통이다(2점)’, ‘대체로 그렇지 않다(1점)’, ‘매우 그렇지 않다(0점)’로 평가되며 검사 결과는 총점과 각 영역별 점수로 산출된다. 설문지에는 환자용 및 보호자/간병인 용으로 나뉘는데 환자용에서 24점 이상일 때 보호자용에서 22점 이상의 경우 인지 저하가 유의한 것으로 해석된다. 다만 환자용의 경우 우울증과 같은 기분 장애에 영향을 받기 때문에 해석의 제한이 있고 보호자용의 민감도가 더욱 높은 것으로 나타났다.6
Brief international cognitive assessment for multiple sclerosis (BICAMS): 다발경화증 간이 국제 인지 평가
BICAMS는 비교적 짧은 시간인 20분 내외로 수행 가능하고 symbol digit modality test (SDMT), 캘리포니아 언어적 학습 과제 2판(California verbal learning test-II, CVLT-II) 및 간편 시공간기억검사 개정판(brief visuospatial memory test-revised, BVMT-R) 총 3가지 하위 검사로 구성된다.8 각 하위 검사에서 얻은 점수를 표준화하여 평가하고 표준화된 점수는 연령, 성별, 교육 수준과 같은 인구 통계학적 변수를 고려하여 비교한다. 하위 검사를 살펴보면 SDMT 검사의 점수는 MS 환자에서 인지적 속도 저하를 감지하는 데 매우 민감하며 병의 진행 상태와도 밀접한 연관이 있다.8 CVLT-II 검사는 언어적 학습 능력과 기억력을 평가하는 과제로 16개의 단어로 구성된 목록을 5회 반복한 뒤 각 회차마다 기억나는 단어를 회상한다. 그리고 20분 뒤 지연 회상 단계에서 단어 목록을 다시 회상하는 방식으로 기억의 저장 및 재인 과정의 손상을 구별하는데 유용한 도구이다. BVMT-R 검사는 시공간 학습 및 기억을 평가하는 과제로 특정한 도형 세트를 10초 동안 제시한 후 기억나는 도형을 그리도록 요청하는 방식으로 3회의 반복 학습 및 지연 회상을 평가하여 비언어적 기억 및 시공간 처리 능력 저하를 평가하며 이는 후두엽과 관련된 기능 손상을 감지하는데 효과적이다. BICAMS는 여러 언어로 표준화되어 있지만 공식적으로 표준화된 한국어 버전은 아직 발표되지 않았다.
Paced auditory serial addition task (PASAT): 청각 연속 과제
PASAT 검사는 외상성 뇌 손상(traumatic brain injury)이 인지 기능에 미치는 영향을 평가하기 위해 개발되었고 다양한 인지 장애를 탐지하는데 임상적으로 유용하다.9 이 과제는 후술할 다발성경화증 기능 종합 척도(minimal assessment of cognitive function in MS, MACFIMS)의 하위 검사에 포함되어 있고 질병 모니터링 및 임상 시험에서의 인지 평가 도구로 사용되어 왔다.10 검사 방법은 청각 자극을 이용하여 주의력, 처리 속도, 계산 능력을 함께 평가하며 2초 혹은 3초마다 한자리 숫자가 녹음된 음성으로 제시되고 수검자는 그 숫자를 바로 직전의 숫자와 더해야 한다. 총 60번의 덧셈을 시행하며 10-15분 내외로 비교적 짧은 시간에 정상군과 MS 환자를 구별할 수 있는 민감도가 높은 검사이지만 임상적으로 유의한 인지 저하를 의미하는 점수가 명확하지 않고 과제가 환자에게 스트레스를 유발하며 교육 수준 및 연령과 같은 다양한 요인에 영향을 받는다.10 PASAT는 다발성 경화증 환자의 인지 기능 평가에 널리 사용되지만 공식적으로 표준화된 한국어 버전은 아직 발표되지 않았다
SDMT: 기호 숫자 양식 검사
SDMT 검사는 처리 속도 및 시각적 작업 기억력을 평가한다. 검사 방법은 검사지 상단에 1부터 9까지 숫자와 기호가 일치하는 시각 자극을 보고 90초 동안 가능한 빠르고 정확하게 제시된 각 기호에 대한 올바른 숫자를 적는다.11 검사 방법이 쉽고 저렴하며 MS 환자들에게서 인지 저하를 감지하는데 민감한 것으로 알려져 있고 검사 점수가 MRI 결과에서 뇌 병변 부하(lesion load), 심실 부피(ventricular volume), 회백질 위축 정도(cortical and deep gray matter atrophy)와도 유의한 상관관계를 보였다.10 이 검사는 단 5분만 소요되며 시행을 위한 특별한 신경 심리학적 훈련이 필요하지 않아 효율적이고 국제적으로 널리 사용되는 인지 검사 도구이지만 처리 속도 외의 다른 인지 영역에 대한 정보를 제공하지 못하는 단순한 검사이며 한국인을 대상으로 공식적으로 표준화된 버전은 아직 발표되지 않았다.10
Mini-mental state examination (MMSE): 간이 정신 상태 검사
MMSE 검사는 가장 널리 쓰이는 도구로 인지 장애의 심각성과 진행률을 추정할 수 있다.12 시간 지남력, 장소 지남력, 기억 등록 및 회상, 언어 및 시공간 구성 능력을 30점 만점으로 평가하며 소요 시간은 10분 내외로 주로 치매의 조기 진단 및 진행을 파악하기 위해 사용되어 인지 기능을 수치화할 수 있는 장점이 있다. 국내에서는 1989년 처음으로 표준화되어 Korean mini-mental state examination 검사로 불리면서 치매 검사에 이용되었고 1998년 원안에 충실하게 번안한 K-MMSE가 만들어져 표준화되었다.13 2020년에는 K-MMSE 검사가 개정되어 K-MMSE-2가 개발되어 표준화되었고 단축형과 확장형을 추가하였으며 동등성이 입증된 두 개의 병렬 검사를 개발하여 연습 효과를 방지하며 반복 검사가 용이하도록 개선되었다.14 MMSE는 MS 환자의 인지 기능 저하를 평가하는 데 민감도가 낮은 편이다. 이는 MMSE 점수가 정상 수준이었던 많은 환자가 다른 종합적인 신경 심리 검사에서는 심각한 인지 장애를 보였다는 연구 결과에서 확인된다.15 나아가 MMSE는 MS에 의해 발생하는 인지 기능 저하를 진단하기에 충분히 민감하지 않으며 비교적 경미한 신체 장애를 가진 재발-완화형 환자에서만 일부 유용성이 보고되었다.15
Montreal cognitive assessment (MoCA): 몬트리올 인지 평가
MoCA 검사는 경도인지 장애(mild cognitive impairment) 16를 MMSE 보다 더 정확하게 변별할 목적으로 개발된 검사로 집행 기능(기호잇기 검사, 공통성 문제, 음소유창성), 시공간 구성 능력(육면체 그리기, 시계 그리기), 기억력(지연 회상), 주의 집중 능력(숫자 외우기, 박수치기, 100에서 7빼기), 언어 기능(대면이름대기, 따라 말하기 및 지남력)으로 구성되어 있고 총점은 30점, 절단 점수는 26점으로 전두엽 기능을 민감하게 평가한다.17 국내에서는 MoCA의 기본틀을 유지하면서 한국인의 문화와 언어적 특성에 맞게 수정하여 Korean-MoCA로 표준화되었다.18 여러 연구를 통해 MoCA는 포괄적 신경 심리 검사를 대체할 수 없지만 MS 환자의 인지 기능 저하를 선별하는 데 효과적임이 입증되었다.19 특히 MoCA 점수는 MS 환자의 뇌 백질 병변 부피와 같은 MRI 지표와 유의미한 상관관계를 보인다는 연구 결과도 발표되었기 때문에,19 특이적으로 백질 병변에 의한 인지 장애가 잘 생길 수 있는 MS 환자들에게도 적용될 가능성이 제시되기도 한다.
종합 심리 평가(comprehensive neuropsychological test, full-battery assessment)
종합 심리 검사는 환자의 전반적인 심리 상태와 특정 문제를 심층적으로 이해하고 정확한 진단과 치료 계획 수립을 위해 사용한다. 포괄적이고 심층적인 검사로 인지, 정서, 성격 및 행동 등을 평가하며 문제의 특성과 환자 상태에 따라 필요한 검사들로 구성된다. 선별 평가에 비해 시간이 오래 걸리고 결과 분석도 복잡하며 장애의 진단, 심각도, 원인 및 특성을 함께 이해할. 수 있다. 가장 많이 사용되는 종합 심리평가 도구는 다음과 같다(Table 2).
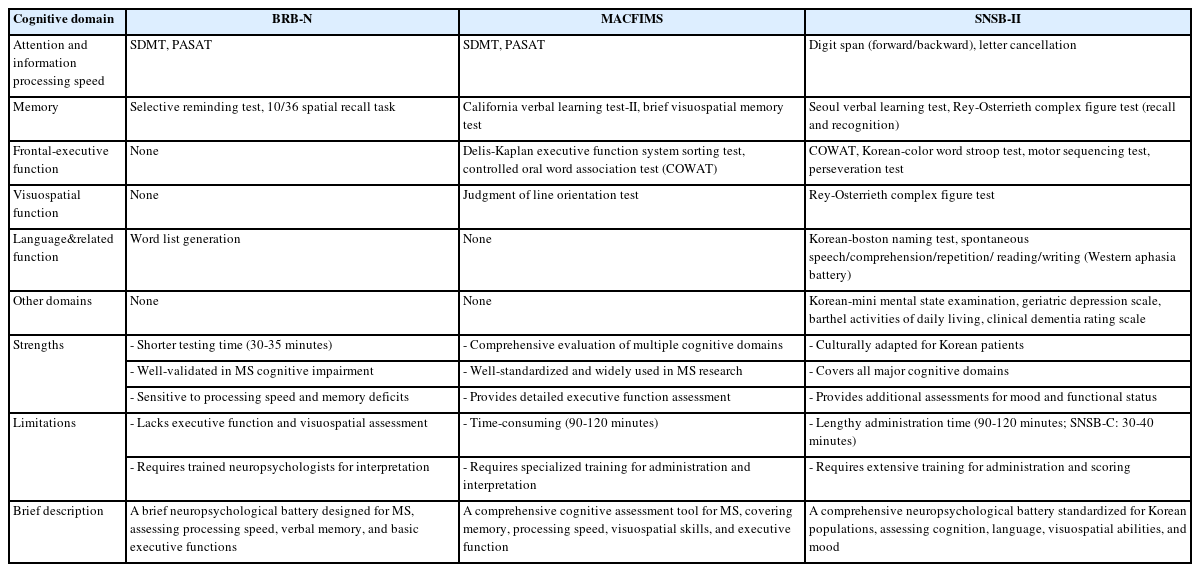
Detailed comparison of cognitive test batteries in multiple sclerosis and SNSB-II
Brief repeatable battery of neuropsychological test (BRB-N) 간이 반복형 신경 심리 검사 배터리
BRB-N 검사는 선별 평가에서 상기한 SDMT 및 PASAT 검사와 더불어 선택적 장기 검사(selective reminder test, SRT), 10/36 공간회상과제(10/36 spatial recall task, SPART), 단어 목록 생성(word list generation, WLG)으로 총 5가지 하위 검사로 구성되어 있고 30-35분 정도 소요되며 평가 및 해석은 신경 심리학 지식을 갖춘 전문가가 필요하다.20 SRT는 언어적 기억력과 학습 메커니즘을 확인하기 위해 단어 목록을 여러 번 반복해서 외운 후 즉각 및 장기 회상 능력을 평가한다. SPART는 시공간 기억력을 평가하는 과제로 무작위로 배열된 10개의 점의 위치를 기억한 뒤 기억한 점의 위치를 빈 격자판에 다시 표시하는 방식으로 진행되며 이를 통해 단기 공간 기억, 학습 능력, 지연 회상 및 오류 분석 등을 함께 파악할 수 있다. WLG는 주로 전두엽과 관련된 언어 및 사고 조직 능력을 측정하는 과제로 언어적 유창성(verbal fluency), 인지적 유연성(cognitive flexibility), 집행 기능(executive function)을 평가한다. 일반적으로 범주적 유창성(categorical fluency)과, 음소적 유창성(phonemic fluency)의 두 가지 유형을 평가하여 총 단어 개수, 군집화(clustering), 다른 군집으로 넘어가는 능력 전환(shifting) 능력 등을 평가하며 짧은 시간 내에 인지 기능에 대한 많은 정보다 정량적 데이터를 얻을 수 있다. BRB-N은 MS 환자의 인지 기능 저하를 선별하는데 효과적이며 작업 기억, 언어 기억, 정보 처리 속도 저하와 같은 핵심적 인지 영역의 손상 패턴을 파악하는데 유용한 것으로 나타났으나 BRB-N은 현재까지 공식적으로 한국어로 표준화된 버전이 발표되지 않았다.21
MACFIMS: 다발경화증 인지 기능 최소 평가 배터리
MACFIMS는 다발경화증 환자의 인지 기능을 심층적으로 평가하기 위해 설계된 검사 배터리로 소요 시간은 약 90-120분이며 총 7개의 하위 검사로 구성되어 있으며 각 검사마다 평가하는 인지 영역이 명확하게 구분된다.22 각 검사는 SDMT, PASAT, CVLT-II, BVMT-R, controlled oral word association test (COWAT), judgment of line orientation (JLO), Delis-Kaplan executive function system sorting test (D-KEFS Sorting Test)이다. COWAT 검사는 WLG 검사와 유사한 양식으로 언어적 유창성과 집행 기능을 평가하는 과제로 구성된다. 주어진 알파벳(예: F, A, S; 한국: ㄱ, ㅇ, ㅅ)으로 시작하는 단어와 특정 범주(동물, 가게 물건)에 속하는 단어를 각각 1분의 제한 시간 내에 최대한 많이 생성한다. JLO 검사는 시공간 능력을 평가하는 과제로 서로 다른 각도로 배열된 선을 보고 기준 선과 동일한 각도의 선을 선택하는 과제이다. D-KEFS Sorting Test는 집행 기능과 문제 해결 능력을 평가하는 과제로 제시한 카드들을 특정 기준에 따라 분류하며 규칙을 유추하고 변경해야 하므로 추론 능력과 유연성이 요구된다. MACFIMS를 사용한 연구 결과에서 MS 환자들의 약 50%가 인지 기능 저하를 보였고 특히 정보 처리 속도와 일화 기억(episodic memory)의 결함이 가장 두드러졌으며 MACFIMS의 여러 하위 검사들이 환자의 직업 유지 여부를 예측하는데 중요한 역할을 한다는 것을 밝혀냈다.22 MACFIMS의 한국어판은 공식적으로 표준화되지 않았다.
Seoul neuropsychological screening battery-II (SNSB-II): 서울 신경 심리 검사 2판
SNSB-II23는 2003년 개발된 SNSB 검사24의 개정판으로 기존 검사 항목을 유지하면서 최신 연구 결과를 바탕으로 새로운 검사를 추가하고 한국인의 대규모 표본 자료를 기반으로 더욱 세부적이고 정확한 규준이 제공되어 기존의 평가 범위를 확장하여 2012년부터 사용 중이다.25 SNSB는 한국인의 문화 및 언어 특성을 반영한 인지 기능 종합 평가 배터리 검사로 경도인지 장애, 치매, 뇌졸중, 뇌 손상, 신경퇴행성 질환과 같은 신경학적 상태를 평가하고 검사의 정량적 점수 및 정성적 관찰을 기반으로 환자의 연령, 학력, 성별에 따른 표준화된 규준을 비교하여 인지적 손상 여부와 심각도를 판별하며 신경 심리학적 프로파일을 제공하여 특정 질환과 연관된 인지적 패턴을 확인할 수 있다. 검사는 총 다섯 개의 주요 인지 영역(기억력, 언어 능력, 시공간 능력, 주의 집중력 및 전두엽 기능)과 정서 평가로 구성된다. SNSB-II에서 시계 그리기(clock drawing test), digit symbol coding 및 Korean-trail making test-elderly’s version 과제가 추가되었다. 또한 개정판에서는 단축형인 SNSB-core (SNSB-C)26를 함께 개발하였다. 단축형에서는 시각적 기억력을 평가하는 지연 회상 과제를 생략함으로써 질문 문항수가 기존 검사와 비교하여 절반 정도로 구성된다. 기존 검사 소요 시간이 90-120분가량 걸리는 반면, 단축형의 경우 30-40분 내외로 소요되어 평가자 및 대상자의 피로도를 줄일 수 있다는 장점이 있다. 물론 국내에서는 알츠하이머병 등 치매 관련 클리닉에서는 검사 비중이 높은 검사이고 다발경화증에 특이적인 검사 항목을 대체할 수 있는 일부 검사를 차용하여 다발경화증이나 시신경척수염범주질환 등의 환자군에서 실시하기도 했지만 질환 특이적 검사 결과는 많이 밝혀지지 않았다.27,28
정서 및 삶의 질 평가
인지 장애를 평가할 때 주요하게 고려해야 하는 대표적인 교란요인(confounder factor)은 정서 상태로 우울과 불안이 가장 중요한 대표적이며 그 외에도 수면 장애 및 피로감을 함께 고려할 수 있다. 우울증은 MS 환자에게서 약 37-54% 정도 발생하며 정상인과 비교하였을 때 4-5배 정도 높은 수치이다. 우울증은 MS 환자들의 작업 기억, 정보 처리 속도, 추상적 추론, 집행 기능 등 여러 인지적 측면에 영향을 미친다.29 우울증 평가에는 diagnostic and statistical manual of mental disorders-530 기준과 Beck depression inventory (벡 우울 척도), hospital anxiety and depression scale, patient health questionnaire, center for epidemiologic studies depression rating scale 및 Hamilton rating scale for depression이 사용된다. MS 연구에서 불안 장애는 우울증과 비교하여 덜 다뤄졌지만 MS 환자들의 불안 장애 유병률은 약 12-40%로 추산되고 피로, 통증, 장애 정도와 관련되며 치료 순응도 저하와 자살 사고 증가로 이어질 수 있다.31 불안을 평가하는 대표적인 설문지로는 Beck anxiety inventory (벡 불안 척도), Hamilton rating scale for anxiety 및 state trait anxiety inventory가 있다. 수면 장애는 MS 환자에게서 약 19-67%에서 보고되며 수면 무호흡과 같은 수면 장애는 정보 처리 속도, 기억력, 주의력, 실행 기능 등을 손상시킨다.5 수면 장애를 평가하는 대표적인 설문지로 Pittsburgh sleep quality index가 있다. 피로감은 MS 환자에게서 70-90%에서 발생하며 일상 기능과 삶의 질을 심각하게 저하시킨다.32 Bakirtzis et al.33은 다발경화증에서 정서적 불편감을 비롯한 피로감과 관련하여 인지 기능 관리를 위한 절차를 제안하였다(Fig. 1).
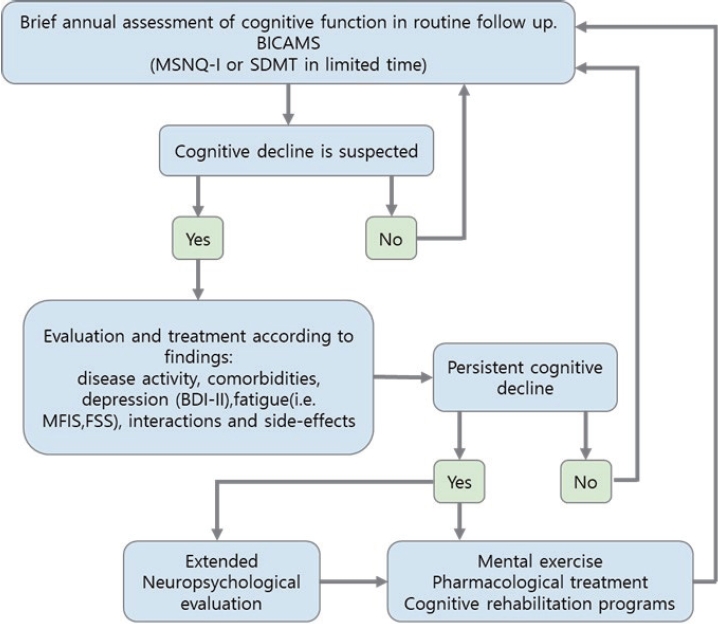
Proposed algorithm for the monitoring of cognitive dysfunction in MS. Adopted from Bakirtzis et al.33 BICAMS, brief international cognitive assessment for multiple sclerosis; MSNQ-I, multiple sclerosis neuropsychological questionnaire informant version; SDMT, symbol digit modalities test; BDI-II, Beck depression inventory-II; MFIS, modified fatigue impact scale; FSS, fatigue severity scale; MS, multiple sclerosis.
세계보건기구(Word Health Organization)는 삶의 질을 개인의 문화적, 사회적 맥락에서 자신의 목표와 기대에 대한 주관적 인식으로 정의하며 이는 신체적, 정신적, 사회적 요인을 포괄하는 광범위한 개념이며 질병이나 장애가 개인의 정상적인 역할을 수행하는 능력에 얼마나 영향을 미치는지 여부와 관련이 있다.34 삶의 질에 대한 평가는 임상 장면에서 주로 다뤄지는 신체 장애 보다 피로, 성 생활 문제, 활력 저하와 같은 측면을 구체적으로 반영하기 때문에 진료에서 미처 발견하지 못한 합병증의 존재를 식별하고 평가할 수 있으며 질병의 임상적 경과를 예측하고 예상하는데 유용하다.35 삶의 질에 대한 평가는 Euro quality of life five-dimension questionnaire (EQ-5D)36와 short form 36 (SF-36)37 설문지 등을 통해 평가된다. EQ-5D는 유럽에서 개발된 삶의 질 측정 도구로 5개의 차원(이동성, 자기 관리, 일상적인 활동, 통증/불편함, 불안/우울감)으로 구성되어 있으며 각 차원은 0-1까지의 점수로 표현되고 한국어 버전도 존재한다. SF-36은 환자들의 신체 건강 및 정신 건강 상태를 측정하는 데 사용되는 자기 보고식 설문지로 신체 기능, 역할 기능, 일반적인 건강, 통증/불편감, 불안/우울증, 사회적 기능, 정서적 안정성 및 체력 수준과 같은 8개의 영역을 평가한다.
다발경화증의 인지 장애 표현형(cognitive phenotype)
Fischer et al.38의 제안에 따르면 다발경화증 환자들에게 실시한 신경 심리학 평가 결과에서 2개 이상의 인지 영역에서 표준편차 점수가 1.5점에 미치지 못하는 경우에 인지 저하가 있는 것으로 정의하였다. MS에서 특정 인지 특성을 식별한 연구는 상대적으로 드물며 일부 연구는 인지 속도나 실행 기능, 에피소드 기억 등 다양한 인지 영역을 포함하여 MS 환자의 인지 상태를 분류하였으나 연구 방법론에 따라 결과가 다르게 나타났다. International classification of cognitive disorders in MS (IC-CoDiMS)는 MS 환자의 인지 장애를 평가하고 분류하기 위해 Hancock et al.39이 개발한 분류 시스템으로 뇌전증 환자의 인지 장애를 분류하기 위해 개발된 International classification of cognitive disorders in epilepsy 모델을 수정 및 확장하여 도입하였다 (Table 3, Fig. 2A). IC-CoDiMS 모델에서는 인지 장애 특성을 총 4가지로 분류하였는데 이는 정상(intact: 손상이 없는 경우), 단일 영역 손상(single-domain impairment: 한 영역에서만 손상된 경우), 이중 영역 손상(bi-domain impairment: 두 영역에서 손상된 경우), 다중 영역 손상(multi-domain impairment: 세 영역 이상에서 손상된 경우)과 같다. 분류 방식은 최소 4개의 인지 영역에 대한 데이터가 있는 환자들을 대상으로 분석했고 인지 영역의 저하 정도는 평균에서 1 표준편차(standard deviation, SD)와 1.5 SD 이하의 기준을 모두 사용하여 정의하였다. 그 결과 1 SD 기준은 더 민감하게 인지적 손상을 탐지하며 경미한 손상까지 확인할 수 있었고 1.5 SD 기준은 임상적으로 더 의미 있는 손상만 걸러내어 대부분의 MS 환자가 정상 인지로 분류되었다. 주된 인지 저하 영역은 주의력/처리 속도, 집행 기능에서 자주 발생했으며 이 두 영역의 결합이 이중 영역 손상(bi-domain impairment)의 가장 흔한 조합이었다.39
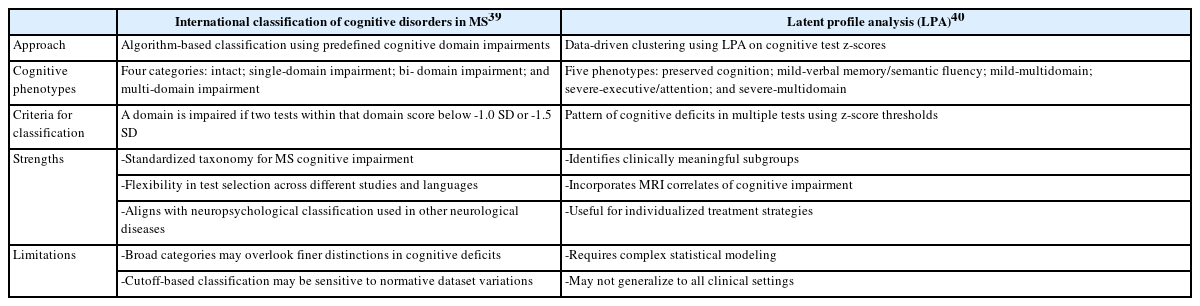
Cognitive phenotypes classification

De Meo et al.40의 연구자들은 대규모 MS 환자 집단의 신경 심리학적 데이터를 잠재 프로파일 분석(latent profile analyses)을 통해 분석하고 MRI 특징을 평가 도구로 확인하였다(Table 3, Fig. 2B). 연구 결과 인지 장애 특성을 총 5가지로 분류하였는데 이는 인지 기능 보존형(preserved cognition), 경미한 언어 기억/유창성 저하형(mild-verbal memory/semantic fluency), 경미한 다영역 저하형(mild-multidomain), 심한 실행 기능/주의 저하형(severe-executive/attention) 및 심한 다영역 저하형(severe-multidomain)과 같다. 인지 기능 보존형의 경우 MRI 결과에서 시상(thalamus)의 부피 감소가 있었고 경미한 언어 기억/의미 유창성 저하형의 경우 SRT 및 WLG 과제 수행 저하가 두드러지며 MRI 결과에서는 해마(hippocampus) 위축과 관련된다. 경미한 다영역 저하형의 경우 SRT, stroop color and word test (SCWT), SDMT, PASAT에서 경미한 저하를 보였다. 심한 실행 기능/주의 저하형의 경우 PASAT 및 SCWT에서 두드러진 저하가 있었으며 MRI 결과에서 백질 병변 부하(white matter lesion load) 증가와 관련이 있다. 심한 다영역 저하형의 경우 모든 인지 검사에서 심각한 저하를 보였고 이는 질병 후기 단계에서 더 빈번했지만 초기 MS 환자에게도 관찰되며 MRI 결과에서 대뇌의 모든 영역에서 심한 위축이 발견되었고 특히 이 집단은 우울증과도 연관이 있었으며 이는 작업 기억, 집행 기능 및 정보 처리 속도 저하 와도 관련 있었다.41
결론
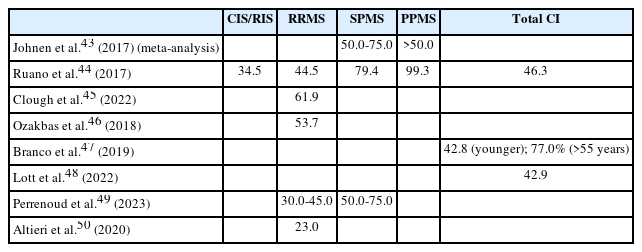
MS는 중추신경계의 염증성 탈수초 질환으로 환자의 약 40-70%에서 인지 장애가 보고되며 아형(subtype) 간에는 인지 기능 장애의 양상이 상당히 다르게 나타난다(Table 4).42 주요 인지 장애는 주의력, 처리 속도, 기억력, 집행 및 실행 기능(전두엽) 저하로 나타나며 이러한 문제는 환자의 일상생활과 직업적 활동에 부정적인 영향을 미친다. 또한 피로, 우울증, 불안 같은 심리적 요인이 인지 기능 악화에 기여할 수 있다. MS 환자의 인지 장애 관리는 정기적인 인지 기능 평가를 통해 약물 치료뿐만 아니라 인지 재활, 심리적 지원 등을 포함한 다학제적 접근이 필요하다.42
인지 장애 평가는 선별 평가와 종합 평가를 통해 확인할 수 있으며 이러한 인지 장애와 심리적 평가는 질병의 전반적인 임상 경과를 이해하고 관리하는 데 있어 핵심적인 역할을 한다. 인지 평가를 통해 질병이 신경계에 미치는 영향을 객관적으로 측정할 수 있으며 이는 질병 진행과 치료제의 유효성을 평가하는 중요한 도구로 사용된다. 또한 우울 및 불안과 같은 심리적 요인은 MS 환자의 정서적 상태와 삶의 질에 밀접한 영향을 미치며 치료와 재활의 성공 가능성을 결정짓는 중요한 변수로 작용한다. 따라서 MS 환자들을 관리할 때 인지 기능과 심리적 상태를 통합적으로 평가하고 이를 기반으로 맞춤형 치료 계획을 수립하는 것은 환자의 삶의 질을 향상시키는 데 필수적이다.
최근 연구에서는 MS 환자의 인지 장애를 세분화하여 다양한 표현형을 구분하려는 시도가 이루어지고 있다. 이러한 인지 장애 표현형의 구분은 환자의 개별적인 신경 인지적 특성을 이해하고 질병의 경과를 예측하며 맞춤형 치료 계획을 수립하는 데 중요한 단서를 제공한다. 특히 특정 표현형이 질환의 진행 과정에서 나타나는 신경퇴행성 변화나 염증 반응과 어떤 관계를 가지는지 밝히는 연구는 장기적인 인지 장애 경과를 이해하는 데 핵심적인 역할을 한다. 이를 통해 MS의 질환 과정을 보다 세부적으로 이해하고 환자의 삶의 질을 높이는 치료법 개발로 이어질 수 있고 이러한 후속 연구는 MS의 임상적, 신경학적 관리에서 새로운 패러다임을 제시할 수 있을 것으로 기대된다.
Notes
Acknowledgements
None.
Author Contributions
Conceptualization: all authors. Formal analysis: all authors. Visualization: all authors. Methodology: all authors. Project administration: SIO. Writing-original draft: all authors. Writing-review & editing: all authors.
Conflicts of Interest
The authors declare no conflicts of interest.
Funding Statement
None.
Data Availability Statement
Not applicable.
Ethical Approval
Not applicable.
Patient Consent for Publication
Not applicable.