국내 다발경화증 역학 조사: 2025년 전국 다기관 병원 기반 연구
Real-World Epidemiology of Multiple Sclerosis in Korea: Insights from a 2025 Nationwide Hospital-Based Multicenter Study
Article information
Trans Abstract
Background
A hospital-based survey conducted in 2023 provided initial insight into the realworld landscape of multiple sclerosis (MS) care. Based on 2023 survey, the present study aims to offer an updated nationwide assessment of MS in Korea.
Methods
In January 2025, we collected data on the number of patients with MS, MS subtypes, newly diagnosed cases in the past year, onset age, sex ratio, current disease modifying therapies (DMTs), and disability status (expanded disability status scale, EDSS) from 47 major MS centers in Korea.
Results
A total of 1,799 patients had clinically confirmed MS and 365 patients were under follow-up for suspected MS. 193 patients were newly diagnosed in 2024. MS onset occurred most frequently at 20-29 years, whereas very early or late onset was uncommon. DMTs were administered to 95% of patients, with 62% receiving moderate-efficacy agents and 28% receiving high-efficacy agents. A majority of patients (78.1%) were followed at centers in the Seoul Capital Area, which also accounted for 79.9% of those receiving high-efficacy therapies. Regarding neurological disability, 307 patients (17%) had an EDSS score greater than 3.0, and 115 patients (6%) had a score above 5.5, indicating moderate to severe disability.
Conclusion
This updated nationwide hospital-based survey reveals a gradual increase in the number of patients with MS under clinical follow-up compared to a 2023 survey conducted in April 2022. The vast majority of patients are receiving DMTs, and while the proportion receiving high-efficacy agents remains modest, it demonstrates a clear upward trend.
서론
다발경화증(multiple sclerosis, MS)은 중추신경계를 침범하는 자가면역 매개 염증성 뇌 질환으로 국내에서는 비교적 드문 질환으로 알려져 있다.1 그러나 최근 들어 전문의의 질환에 대한 인식 개선, 진단 기술의 발전, 보건 의료 접근성 향상 및 기대수명의 증가 등 다양한 요인으로 인해 MS의 보고 유병률은 점차 증가하고 있는 추세이다. 그럼에도 불구하고 국내에서 MS에 대한 임상적으로 검증된 전국 단위의 역학 자료는 여전히 부족하다. 기존의 국민건강보험공단 자료를 기반으로 한 역학 연구는 실제 임상 진단이 아닌 행정 데이터를 바탕으로 하므로 오진 가능성이 있으며 확진의 정확도에도 한계가 존재한다.2,3 이러한 점을 보완하고자 2023년에는 신경과 전문의를 대상으로 한 병원 기반 설문조사가 실시되어 국내 MS 진료 현황에 대한 초기적인 통찰을 제공한 바 있다.4 본 연구는 해당 선행 연구를 기반으로 하되 이전보다 훨씬 많은 수의 전국 신경과 전문 의료기관이 참여함으로써 국내 MS 진료 현황을 보다 정밀하고 대표성 있게 반영하였다. 이를 통해 신경과 전문의에 의해 임상적으로 확진된 다기관의 환자 데이터를 종합 분석하여 MS 환자의 역학적 특성, 치료 경향, 장애 부담을 심층적으로 고찰하고자 한다. 특히 최근 국내에 도입된 고효능 질환 조절 치료제(disease-modifying therapies, DMTs)의 실제 사용 현황과 그 임상적 함의를 분석함으로써 향후 MS 진료의 질 향상과 효과적인 보건 의료 정책 수립에 토대가 될 기초 자료를 제공하고자 한다. 아울러 본 연구는 국내 MS 진료 및 관리 체계에서의 사각지대를 조명하고, 중장기적인 진료 전략 수립과 표준화된 진료 가이드라인 개발을 위한 근거 자료로도 활용될 수 있다는 데 그 의의가 있다.
대상과 방법
2025년 1월, 우리는 국내 47개 주요 병원들을 대상으로 전국 단면 조사(nationwide cross-sectional survey)를 시행하였다. 이 중 26개는 상급종합병원(tertiary hospitals), 20개는 종합병원(secondary hospitals), 1개는 1차 진료기관(primary care clinic)이었다. 본 연구는 신경과 전문의에 의해 MS로 확진되었거나 MS가 의심되어 추적 중인 환자의 수, MS의 세부 아형(subtypes), 최근 1년간의 신규 진단 사례, 발병 연령, 성별 분포, 질환 조절 치료제 사용 현황, 및 확장 장애 상태 척도(expanded disability status scale, EDSS)5에 근거한 장애 상태를 수집하여 분석하였다. 본 연구에서 MS가 의심되어 추적 관찰 중인 환자는 2017년 개정 McDonald 진단 기준을 완전히 충족하지는 않았으나 임상적·영상학적 소견상 MS 가능성이 높아 신경과 전문의에 의해 지속적인 추적 관찰이 필요하다고 판단된 환자를 의미한다. 이들 환자는 주로 임상적으로 고립된 증후군(clinically isolated syndrome) 또는 영상학적으로 고립된 증후군(radiologically isolated syndrome)에 해당하였으며 일부는 임상적 경과가 짧거나 진단에 필요한 추적 정보가 충분하지 않아 명확한 범주 분류가 어려운 상태였다. DMTs는 전반적인 효과 수준에 따라 선행 연구 및 치료 알고리즘에서 흔히 사용하는 기준에 근거하여 중등도 효과(moderate-efficacy) 치료제와 고효능(high-efficacy) 치료제로 분류하였다. 이러한 분류는 재발률 감소 및 뇌 자기공명영상의 질병 활성 억제 효과의 차이에 기반한 것으로 다발성경화증 치료 전략을 비교한 선행 문헌에서도 널리 사용되고 있다.6,7 또한 MS 적응증으로 공식 승인되지 않았으나 임상적으로 사용된 면역억제제는 off-label immunosuppressants로 정의하였고 임상 시험 프로토콜에 따라 투여된 약제는 clinical trial treatment로 별도로 분류하였다. EDSS 점수는 각 참여 기관에서 조사 시점과 가장 인접한 시기의 임상 진료 과정에서 기록된 최근 값을 사용하였다.
결과
총 1,799명이 임상적으로 확진된 MS 환자였으며 추가로 365명은 MS가 의심되어 추적 관찰 중이었다. MS로 확진된 전체 환자 중 여성 대 남성의 비율은 2.2:1로 여성에서 더 높은 유병률을 보였다. 2024년 한 해 동안 새롭게 진단된 MS 확진 환자는 193명이었다. 발병 연령은 총 1,687명(93.9%)에서 분석하였고 0 -9세 5명(0.3%), 10-19세 170명(9.5%), 20-29세 613명(34.1%), 30-39세 422명(23.5%), 40-49세 302명(16.8%), 50-59세 132명(7.3%), 60-69세 34명(1.9%), 70-79세 9명(0.5%)이었다(Fig. 1). 임상 아형별 분포는 재발-완화형 다발경화증(relapsing-remitting MS)이 92%로 가장 많았으며 속발 진행형 다발경화증(secondary progressive MS)이 6%, 원발 진행형 다발경화증(primary progressive MS)이 2%를 차지하였다. DMTs는 전체 환자의 95%인 1,709명에서 사용 중이었으며 치료를 받고 있는 1,709명의 환자 중에서 1,116명(65.3%)은 중등도 효과의 DMTs (interferon beta-1a, interferon beta-1b, peginterferon-1a, glatiramer acetate, teriflunomide, and dimethyl fumarate)를, 512명(29.9%)은 고효능 DMTs (fingolimod, cladribine, natalizumab, alemtuzumab, and rituximab)를 투여 받고 있었다. 나머지 81명(4.7%)은 임상시험에 참여하거나 표준 DMTs 범주에 포함되지 않는 기타 면역억제 치료(azathioprine, mycophenolate mofetil, tacrolimus, and cyclosporine)를 받고 있었다(Table 1). 중등도 효과의 약물을 복용하는 1,116명 중 경구 약제의 사용 빈도는 67%로 자가주사제 사용 빈도 33%보다 높았으며 고효능 약물 중에서는 cladribine 사용이 54%로 가장 높았고 fingolimod가 26%로 그 뒤를 이었다. 지역별 분포를 살펴보면 전체 환자의 78.1%는 수도권(서울, 경기 및 인천지역) 의료기관에서 추적 관찰 중이었으며(Fig. 2), 고효능 DMTs 사용 환자의 79.9% 또한 수도권에 집중되어 있어 고도 진료 접근성에서 지역 간 차이가 있음을 시사하였다(Fig. 3). 지역별로 세부 분석했을 때 고효능 DMTs를 사용 중인 환자의 비율은 서울에서 44.7%로 가장 높았고 경기가 34.8%로 그 뒤를 이었다. 서울 및 경기 지역을 제외한 나머지 지역에서는 최소 0.4%에서 최대 7.4%의 고효능 DMTs 사용 분포를 보였다. 신경학적 장애 정도는 전체 환자 중 307명(17%)이 EDSS 3.0 초과, 115명(6%)이 EDSS 5.5 초과로 확인되어 중등도 이상의 장애를 보였다.
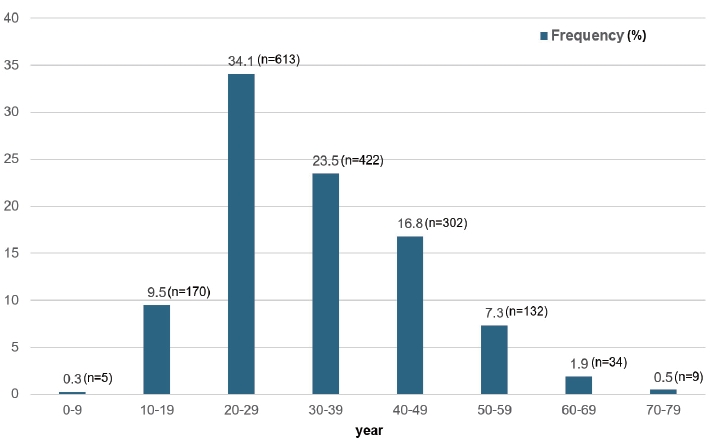
Distribution of age at multiple sclerosis onset in the study cohort. Among 1,687 patients with available onset age data (93.9% of the cohort), the highest frequency was observed in the 20-29-year age group (613 patients; 34.1%), followed by 30-39 years group (422 patients; 23.5%) and 40-49 years group (302 patients; 16.8%). Onset before age 10 (five patients; 0.3%) or after age 70 (nine patients; 0.5%) was uncommon.
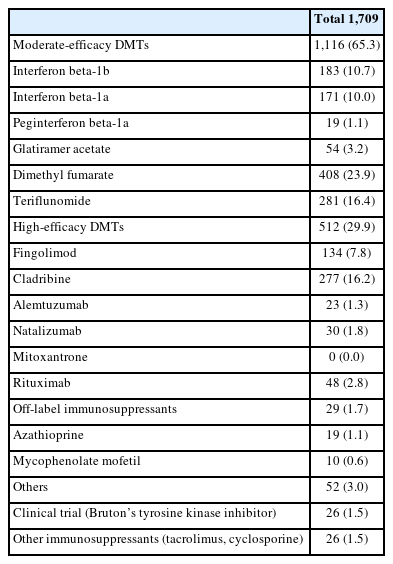
Type of disease-modifying therapies (DMTs) currently used in South Korea patients with multiple sclerosis
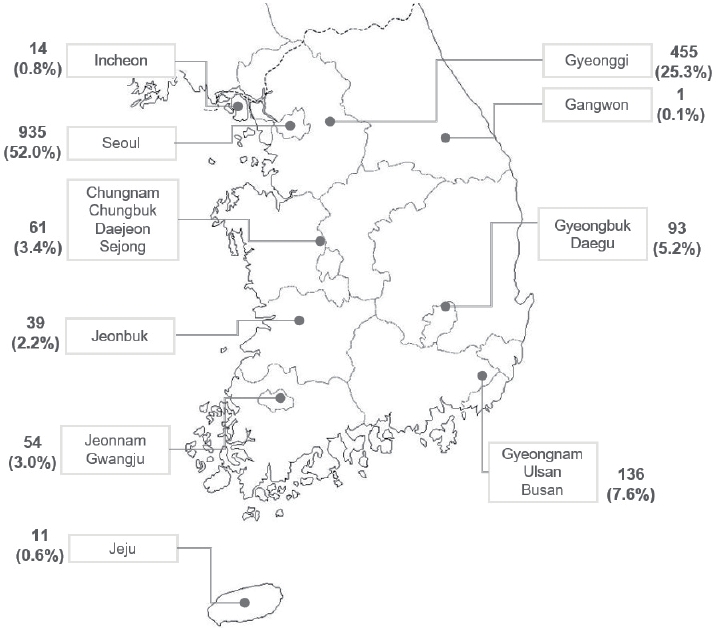
Regional distribution of currently followed patients with clinically confirmed multiple sclerosis across South Korea. The highest number of cases were reported in Seoul, followed by Gyeonggi Province and Gyeongnam/Ulsan/Busan. The majority of patients (78.1%) were treated at centers located in the Seoul Metropolitan area (Seoul, Incheon, and Gyeonggi Province). Data were obtained from a nationwide hospital-based survey conducted in January 2025.
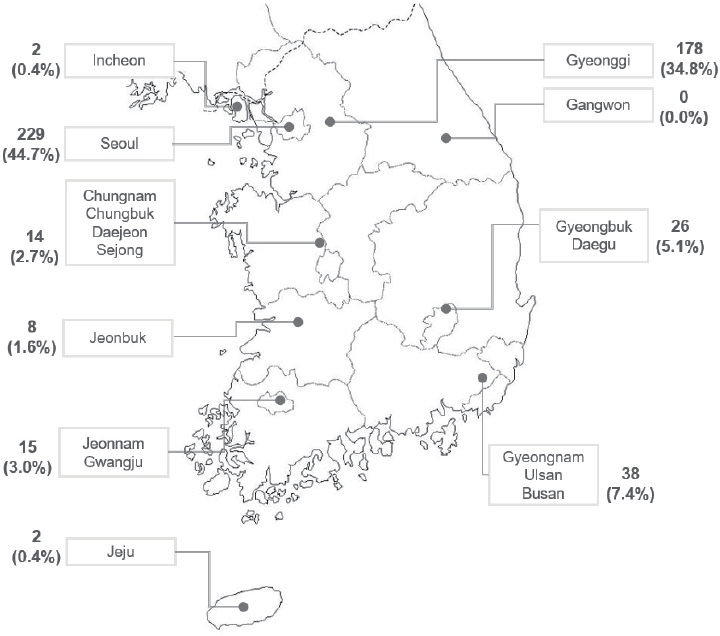
Geographic distribution of patients with multiple sclerosis receiving high-efficacy disease-modifying therapies (DMTs) across South Korea. The highest concentrations were observed in Seoul (n=229), Gyeonggi and Incheon Province (n=180), and Gyeongnam/Ulsan/Busan area (n=38). Notably, 79.9% (n=409) of all high-efficacy DMTs recipients were managed at centers in the Seoul Metropolitan area (Seoul, Incheon, and Gyeonggi Province).
고찰
본 연구는 2023년 보고된 전국 단면 조사의 후속 연구로서 신경과 전문의에 의해 확진된 MS 환자의 임상적 특성과 치료 경향, 장애 부담 및 치료의 지역별 분포를 보다 확장된 규모에서 재확인하였다. 선행 연구보다 참여 기관의 증가를 통해 연구의 신뢰도를 향상시켰으며 이는 전국 단위 환자 관리의 실제적 변화를 반영하였다고 판단된다. 이번 연구는 선행 연구를 토대로 하여 국내 MS 진료 양상의 변화를 시계열적으로 살펴볼 수 있다는 데에 의의가 있으며 특히 신경과 전문의에 의해 임상적으로 확진된 환자만을 대상으로 하였다는 점에서 질병코드 및 산정특례 코드로 추출하는 건강보험공단 데이터 기반 연구가 지니는 잠재적인 오진 가능성과 진단 정확도의 한계를 보완한다는 강점을 지닌다. 2022년 보고된 건강보험공단 데이터 기반 역학 연구에서는 MS에서 뇌졸중 위험성을 분석하였고 해당 연구의 역학 조사에서는 국내 MS 환자가 2,515명으로 산출되었다.6 이에 비하면 본 연구의 확진 MS 환자가 더 적게 관찰되나 이는 건강보험공단 데이터 기반 역학 연구에서 MS가 아닌 다른 유사 질환의 환자가 혼재되어 있을 가능성이 있고 본 연구가 국내 47개의 주요 의료기관에서 확진된 MS 환자를 분석하였으나 모든 의료기관의 환자를 분석한 것이 아니므로 일부 누락되었을 가능성이 있다. 따라서 향후 국내 MS 환자의 정확한 유병률 확인을 위해서는 신경과 전문의 대상 환자 등록 네트워크를 구성 및 유지하고 참여기관을 확대하는 방안을 검토하는 것이 필요하다.
2023년 보고된 선행 설문 연구에서는 전국 30개 주요 MS 진료기관을 대상으로 시행된 조사에서 총 1,290명의 확진 환자가 확인되었으며 이 중 새로이 진단된 환자는 183명이었다.
본 연구에서는 참여 병원이 이전보다 크게 확대되어 전국 대부분의 주요 신경과 의료기관이 포함되었으며 이에 따라 조사에 반영된 환자 수는 1,799명으로 증가하였고 이는 본 연구에 참여한 병원 기반 조사에서 포착된 환자 수를 기준으로 할 때 대한민국 총 인구 대비 10만 명당 약 3.5명에 해당하는 수준이다. 새로이 확진된 환자 수(약 193명)는 선행 연구와 유사하였으나 전체 환자 수의 증가는 조사에 참여한 의료기관의 확대와 선행 연구 이후 2년간 축적된 신규 환자들의 반영이 주요 요인으로 작용한 것으로 판단되며 그 외 질환에 대한 인식 향상, 접근성 개선 등이 일부 영향을 미쳤을 가능성도 있다. 임상 아형 분포에서 재발-완화형이 대부분을 차지하였고 여성 우세가 확인되었다. 이는 기존 국내외 보고와 일관된 결과였다.7-9 DMTs 사용 양상에서 중등도 효과 약제의 비율은 선행 연구와 유사하였으나 고효능 약제 내 구성에는 뚜렷한 변화가 관찰되었다. 선행 연구에서는 fingolimod가 가장 많이 사용된 반면 본 연구에서는 cladribine이 가장 높은 비율을 차지하였다. 이는 경구 고효능 약제에 대한 접근성 확대뿐 아니라 투약 일정이 단기적이고 복용이 간편하여 환자 순응도가 높은 cladribine의 특성이 선호도 변화에 기여한 것으로 해석된다. 고효능 DMTs 사용 비율은 선행 연구의 22%에서 본 연구의 28%로 증가하였다. 이러한 증가는 고효능 약제에 대한 접근성 확대와 임상적 선호도의 변화를 반영하는 것으로 보이며 국제 가이드라인에서 제시하는 조기 고효능 치료 전략의 확산이 일정 부분 영향을 미친 것으로 판단된다.10-13 본 연구 종료 이후 2025년 3월부터 고효능 DMTs인 오크렐리주맙이 급여화되어 임상 현장에서 사용이 증가할 것으로 예상되며 향후 Bruton’s tyrosine kinase 억제제와 같은 새로운 약제 도입은 국내 MS 치료에 더욱 큰 변화를 가져올 것으로 예상된다.
이번 연구에서 주목할 만한 또 다른 결과는 MS 치료의 수도권 집중 현상이다. 2023년 선행 연구와 마찬가지로 국내 MS 진료는 여전히 수도권에 과도하게 집중되어 있었다. 전체 환자의 약 78.1%가 수도권 의료기관에서 추적 관찰이 되고 있었으며 고효능 DMTs 투여 환자 중 수도권에서 치료를 받는 환자는 전체 치료 환자의 79.9%에 달했다. 특히 서울(44.7%)과 경기(34.8%) 지역에서 사용률이 가장 높았던 반면 일부 비수도권 지역에서는 1% 미만으로 낮았다. 이러한 결과는 단순히 수도권에 인구와 의료 인프라의 집중을 넘어 지역 간 고효능 치료 접근성의 불균형이 존재함을 시사한다. 환자 개인의 수도권 진료 선택도 일부 영향을 미치지만 지역 내 약제 처방 제한, 의료진의 경험 차이, 또는 의사 개인의 선호도 등도 고효능 약제 사용률 격차의 요인으로 작용할 가능성이 있다. MS는 조기 고효능 치료가 장기적인 장애 억제와 삶의 질 유지에 중요한 질환인 만큼 지역 간 접근성 격차는 환자의 예후에 잠재적으로 영향을 미칠 가능성이 있다. 따라서 본 연구의 결과는 학회 차원의 지속적인 교육 강화, 전문가 간 경험 공유를 위한 네트워크 구축, 권역별 거점 센터의 운영 확대 등 체계적 전략을 통해 지역 불균형 해소를 도모해야 함을 시사한다.
본 연구의 제한점은 단면 조사 연구 특성상 인과 관계 해석에는 한계가 있으며 장기 추적 관찰 자료가 없다는 점, 일부 포함되지 않은 MS 환자가 존재할 수 있다는 점을 들 수 있다. 하지만 본 연구는 신경과 전문의에 의해 확진된 MS 환자를 대상으로 하였으며 전국의 모든 지역이 포함된 전국 단위 임상 기반 분석 연구라는 점, 선행 조사와 동일한 방법론을 적용하여 시계열적 비교가 가능하다는 점에서 의미가 있다고 판단된다. 본 연구가 2023년 연구의 후속 연구인 것과 같이 국내 MS 역학 조사를 위한 이러한 전문가 네트워크 기반 역학 조사가 지속적으로 업데이트되어야 하며 이러한 노력은 국내의 실정에 맞는 MS 진료 지침 및 정책 개발의 기초 자료가 될 수 있을 것이다. 또한 향후에는 국가 단위 레지스트리 구축을 통해 환자의 장기적인 임상 경과 및 치료 효과, 삶의 질 및 경제적 부담을 종합적으로 평가할 필요가 있으며 아울러 새로운 고효능 약제의 도입과 함께 지역 간 불균형을 줄이는 정책적 노력이 병행될 때 국내 MS 환자 진료의 수준을 더욱 향상시킬 수 있을 것이라 전망된다.
Notes
Acknowledgements
None.
Author Contributions
Conceptualization: SK, HJK, SHK. Data curation: SK, SHK. Investigation: all authors. Methodology: HJK, SHK. Project administration: HJK, SHK. Supervision: SHK. Validation: SK, SHK. Writing-original draft: SK. Writing- review & editing: all authors.
Conflicts of Interest
There is no conflict of interest.
Funding Statement
This research received no specific grant from any funding agency in the public, commercial, or not-forprofit sectors.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to institutional restrictions and the aggregated nature of the survey.
Ethical Approval
This study was conducted using aggregated, anonymized survey data collected from participating centers and did not involve direct patient contact or identifiable personal information. Therefore, ethical approval and informed consent were waived in accordance with local regulations.
Patient Consent for Publication
Not applicable.