항종양괴사인자 치료 중인 크론병 환자에서 대뇌피질뇌염으로 발현한 MOG항체 연관 질환
Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease Presenting as Cortical Encephalitis in A Patient with Crohn’s Disease Receiving Anti-Tumor Necrosis Factor Therapy
Article information
Trans Abstract
A 28-year-old man with Crohn’s disease receiving infliximab developed focal motor seizures with unilateral cortical hyperintensity on brain magnetic resonance imaging and serum myelin oligodendrocyte glycoprotein (MOG)-immunoglobulin G positivity, consistent with MOG antibody-associated disease (MOGAD) presenting as cortical encephalitis. His symptoms improved after corticosteroid therapy. MOGAD should be considered in patients receiving anti-tumor necrosis factor therapy who develop new-onset cortical manifestations.
Cortical encephalitis is a recognized manifestation of myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD), characterized by seizures and unilateral cortical fluid-attenuated inversion recovery (FLAIR) hyperintensity.1,2 Although anti-tumor necrosis factor (TNF) therapy has been associated with central nervous system (CNS) demyelinating events, its relationship with MOGAD remains unclear.3 We report a patient with Crohn’s disease receiving anti-TNF therapy who developed MOGAD presenting as cortical encephalitis.
CASE
A 28-year-old man with Crohn’s disease who had been treated with infliximab every 8 weeks for 2 years presented with recurrent abnormal movements of the left hand. The episodes consisted of intermittent flexion and tremulous movements of the second through fourth digits, lasted several seconds, and occurred multiple times per day. Neurological examination between episodes was unremarkable. Although electroencephalography showed no epileptiform discharges, the events were stereotyped, brief, and recurrent, consistent with focal motor seizures.
Brain magnetic resonance imaging revealed focal FLAIR hyperintensity in the right perirolandic region with subtle enhancement (Fig. 1). Diffusion-weighted imaging showed no definite diffusion restriction. Cerebrospinal fluid analysis revealed no pleocytosis, normal biochemical findings, and no oligoclonal bands. Evaluation for infectious and autoimmune encephalitis, as well as neoplastic and vascular causes, was unremarkable. However, serum MOG-immunoglobulin G (IgG) testing using a live-cell flow cytometry assay (EONE Laboratories, Incheon, Korea) was positive, with a mean fluorescence intensity ratio of 5.33 (positive, >2.61; borderline, 2.02-2.61; negative, ≤2.02). The patient was treated with high-dose intravenous methylprednisolone and no recurrence of symptoms was observed during follow-up.
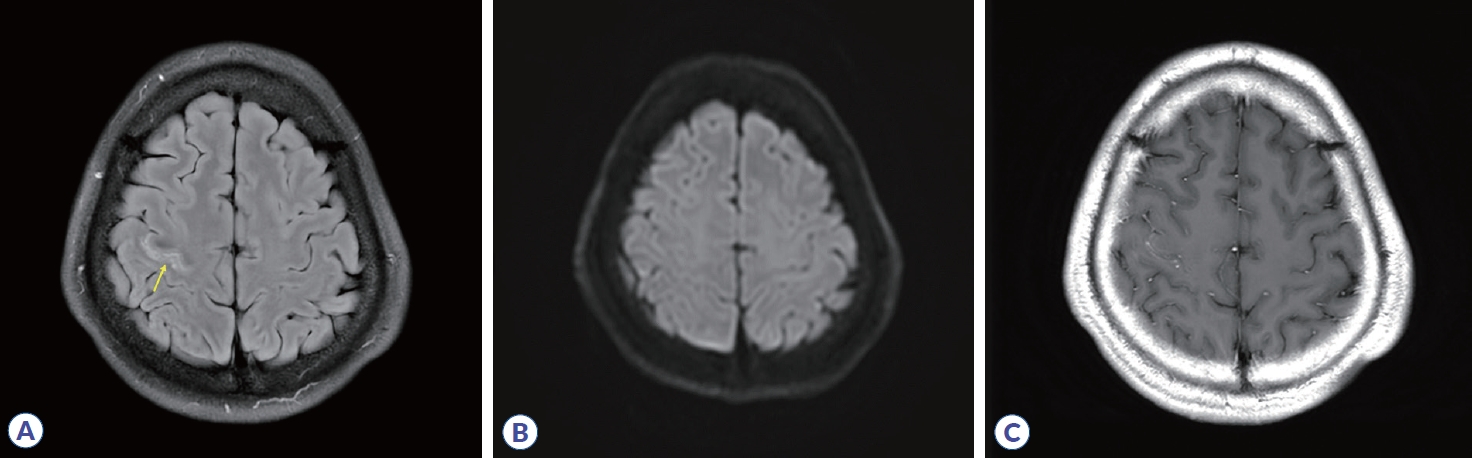
Brain MRI findings of the patient. (A) Axial FLAIR image showing focal hyperintensity in the right perirolandic cortex (arrow). (B) Diffusion-weighted imaging showing no definite diffusion restriction. (C) Post-contrast T1-weighted image demonstrating subtle cortical enhancement without leptomeningeal involvement. MRI, magnetic resonance imaging; FLAIR, fluid attenuated inversion recovery.
DISCUSSION
This case is consistent with the cortical encephalitis phenotype of MOGAD, initially described by Ogawa et al.2 and subsequently characterized by Budhram et al.4 This phenotype, termed FLAIR-hyperintense lesions in anti-MOG-associated encephalitis with seizures (FLAMES), is characterized by focal seizures, unilateral cortical FLAIR hyperintensity, and a favorable response to immunotherapy.
The patient had received infliximab every 8 weeks for 2 years before symptom onset. Although anti-TNF agents are widely used, paradoxical immune-mediated neurological adverse events, particularly demyelinating disorders, have been increasingly recognized.3 Anti-TNF-associated demyelination has primarily been linked to multiple sclerosis-like syndromes; however, emerging evidence suggests that other inflammatory demyelinating disorders may also occur.3 Anti-TNF-associated MOGAD appears to be rare. In the largest available series, exposure to an anti-TNF agent at MOGAD presentation was identified in only a small minority of patients (five of 336 MOGAD cases).5 Reported cases have demonstrated considerable clinical heterogeneity, including cortical encephalitis (FLAMES), optic neuritis, myelitis, and brainstem involvement. These events have been associated with multiple TNF inhibitors, with symptom onset occurring both during ongoing treatment and after discontinuation (Supplementary Table 1).
Proposed mechanisms suggest that anti-TNF-α agents may inadvertently suppress protective and regenerative pathways mediated by TNF receptor 2 in the CNS. In addition, alterations in TNF-mediated immune regulation may reduce the suppressive capacity of regulatory T cells or promote a compensatory increase in the trafficking of autoreactive T cells into the CNS, ultimately contributing to neuroinflammation and demyelination.6 The temporal relationship between symptom onset and infliximab exposure in our patient raises the possibility of an association between TNF inhibition and MOGAD. However, whether TNF inhibitors directly induce MOGAD or unmask an underlying predisposition to CNS autoimmunity remains uncertain.7 The underlying inflammatory bowel disease may also have contributed. Extraintestinal neurological manifestations have been reported in patients with inflammatory bowel disease and shared immune mechanisms may promote CNS autoimmunity.8 Therefore, it remains difficult to determine whether MOGAD in this setting was related to TNF inhibitor exposure, the underlying autoimmune disease, or an interaction between the two. Larger studies are needed to clarify the causal relationships and immunological mechanisms linking TNF inhibitors to the onset of MOGAD.
This case adds to the limited literature on MOGADassociated cortical encephalitis in patients with Crohn’s disease receiving long-term infliximab therapy. It also highlights the importance of considering MOGAD and performing MOG-IgG testing in patients receiving anti-TNF therapy who develop new neurological symptoms.
Notes
Acknowledgements
None.
Author Contributions
Conceptualization: JMS, JHK. Data curation: JMS, JHK. Visualization: JYL. Writing-original draft: JYL, JMS. Writing-review & editing: all authors.
Conflict of Interest
The authors have no potential conflicts of interest to disclose.
Funding Statement
None.
Data Availability Statement
No data are available.
Ethical Approval
This study was approved by the Institutional Review Board of Ewha Womans University Seoul Hospital (#2026-04-075-001). The requirement for informed consent was waived owing to the retrospective nature of the study and the inability to obtain consent because the patient was lost to follow-up.
Patient Consent for Publication
Patient consent for publication was waived by the Institutional Review Board. Care was taken to ensure that no identifiable patient information is included in this report.
Supplementary Material
The Supplementary Material for this article can be found online at: https://doi.org/10.59578/jmsni.2026.17.1.7-10
Supplementary Table 1.
Summary of reported cases of MOGAD associated with anti-TNF therapy