

ņä£ļĪĀ
ļŗżļ░£ņä▒Ļ▓ĮĒÖöņ”Ø(multiple sclerosis, MS) ņ¦äļŗ©ņØĆ ņśżņ¦ü ņżæņČöņŗĀĻ▓ĮĻ│ä ņŚ╝ņ”Øņä▒ Ēāłņłśņ┤ł ĒśäņāüņŚÉ ļČĆĒĢ®ĒĢśļŖö ņ”ØņāüĻ│╝ ņŗĀĻ▓ĮĒĢÖņĀü ņ¦ĢĒøäļ¦īņØä ņØĖņĀĢĒĢśļŖö ņ¦äļŗ© ĻĖ░ņżĆņŚÉņä£ ņŗ£ņ×æĒĢśņŚ¼1 1983ļģä Poser ļō▒2ņŚÉ ņØśĒĢ┤ ļćīņ▓ÖņłśņĢĪ Ēæ£ņ¦Ćņ×É(ņś¼ļ”¼Ļ│ĀĒü┤ļĪĀļØĀ, immunoglobulin G ņ¦Ćņłś)ņÖĆ ņĀäĻĖ░ņāØļ”¼Ļ▓Ćņé¼(ņ£Āļ░£ņĀäņ£ä ļō▒) Ļ░ÖņØĆ ņ×äņāüņ”ØņāüļČĆņåŹĻĘ╝Ļ▒░(paraclinical evidence)Ļ░Ć ņ¦äļŗ© ĻĖ░ņżĆņŚÉ ĒżĒĢ©ļÉśņŚłĻ│Ā ņØ┤Ēøä McDonald ņ¦äļŗ© ĻĖ░ņżĆ(2001-2017ļģä)ļČĆĒä░ļŖö ņ×ÉĻĖ░Ļ│Ąļ¬ģņśüņāü(MRI)ņØ┤ MS ņ¦äļŗ©ņŚÉ ņ׳ņ¢┤ ļ¦żņÜ░ ĒĢĄņŗ¼ņĀüņØĖ ņŚŁĒĢĀņØä ĒĢśĻĖ░ ņŗ£ņ×æĒĢśņśĆļŗż.3-5 MS ĒŖ╣ņØ┤ņĀüņØĖ ņżæņČöņŗĀĻ▓ĮĻ│ä ļé┤ ņŗ£Ļ░äņĀü Ēīīņóģ(dissemination in time, DIT), Ļ│ĄĻ░äņĀü Ēīīņóģ(dissemination in space, DIS) ņ×ģņ”ØņŚÉ ņ׳ņ¢┤ņä£ Ļ░ØĻ┤ĆņĀüņØĖ ņ×äņāüĻĘ╝Ļ▒░ ņÖĖņŚÉ MRI ĻĘ╝Ļ▒░ļÅä ņØĖņĀĢĒĢśĻ▓ī ļÉ£ Ļ▓āņØ┤ļŗż. ņØ┤ļ¤¼ĒĢ£ ņ¦äļŗ© ĻĖ░ņżĆņØś ļ│ĆĒÖöļŖö MS ņ¦äļŗ©ņØś ĒŖ╣ņØ┤ļÅäļź╝ Ēø╝ņåÉĒĢśņ¦Ć ņĢŖņ£╝ļ®┤ņä£ļÅä ļ»╝Ļ░ÉļÅäļź╝ Ē¢źņāüņŗ£ĒéżļŖö ļ░®Ē¢źņ£╝ļĪ£ ņØ┤ļŻ©ņ¢┤ņĪīĻ│Ā, ĒŖ╣Ē׳ McDonald ņ¦äļŗ© ĻĖ░ņżĆņØ┤ Ļ░£ņĀĢņØä Ļ▒░ļōŁĒĢ©ņŚÉ ļö░ļØ╝ ņ▓½ ņ”Øņāü ļ░£ņāØ ņØ┤Ēøä MS ņ¦äļŗ©Ļ╣īņ¦Ć ņåīņÜöļÉśļŖö ņŗ£Ļ░äņØ┤ 2ļģä(Poser ĻĖ░ņżĆ)ņŚÉņä£ 6Ļ░£ņøö(2010 McDonald ĻĖ░ņżĆ)ļĪ£ ļŗ©ņČĢļÉĀ ņłś ņ׳ņŚłļŗż.6 ĻĘĖļ¤¼ļéś ļ»╝Ļ░ÉļÅäĻ░Ć ļåÆņĢäņ¦ĆļŖö ņ¦äļŗ© ĻĖ░ņżĆ Ļ░£ņĀĢņØś ņØ┤ļ®┤ņŚÉļŖö MS ņśżņ¦ä ņ£äĒŚśņä▒ņØ┤ ņ׳ņØīņØä ĒĢŁņāü ņŚ╝ļæÉņŚÉ ļæÉņ¢┤ņĢ╝ ĒĢśļ®░7,8 McDonald ņ¦äļŗ© ĻĖ░ņżĆ ņĀüņÜ® ņŗ£ ņĀäņĀ£ ņĪ░Ļ▒┤Ļ│╝ ņŻ╝ņØśņĀÉņŚÉ ļīĆĒĢ┤ņä£ ņłÖņ¦ĆĒĢśĻ│Ā ņ׳ņ¢┤ņĢ╝ ĒĢ£ļŗż. ņ”ē ņĀäĒśĢņĀüņØĖ ņ×äņāüņĀü ļŗ©ļÅģņ”ØĒøäĻĄ░(clinically isolated syndrome)ņ£╝ļĪ£ ļ░£ĒśäĒĢ£ Ļ▓ĮņÜ░ņŚÉ ĒĢ£ĒĢśņŚ¼ ņĀüņÜ®ĒĢśļ®░, ņ£Āņé¼ņ¦łĒÖśņØä ļ░░ņĀ£ĒĢśĻĖ░ ņ£äĒĢ£ ņ¦äļŗ©ņĀü ņĀłņ░©Ļ░Ć ļ░śļō£ņŗ£ ĒĢäņÜöĒĢśĻ│Ā, Ļ│╝Ļ▒░ ļ│æļĀźņØĆ Ļ░ØĻ┤ĆņĀüņØĖ ņ”ØĻ▒░Ļ░Ć ņ׳ņØä ļĢīņŚÉļ¦ī ņ¦äļŗ© ĻĖ░ņżĆņŚÉ ĒżĒĢ©ĒĢ£ļŗż.5,9
ļ│Ė ņóģņäżņŚÉņä£ļŖö 2017 McDonald ņ¦äļŗ© ĻĖ░ņżĆņŚÉņä£ ņĀ£ņŗ£ĒĢśĻ│Ā ņ׳ļŖö MRI ĻĖ░ņżĆņŚÉ ļīĆĒĢ┤ ņĢīņĢäļ│┤Ļ│Ā, ņĄ£ĻĘ╝ ņŚ░ĻĄ¼Ļ░Ć Ļ▒░ļōŁļÉśĻ│Ā ņ׳ļŖö T2* Ļ░ĢņĪ░ņśüņāü ļ░Å ņ×ÉĒÖöņ£©Ļ░ĢņĪ░ņśüņāü(susceptibility weighted imaging)ņŚÉņä£ņØś MS ĒŖ╣ņØ┤ņĀü ņåīĻ▓¼ņŚÉ ļīĆĒĢ┤ņä£ Ļ░äļץĒ׳ ņĢīņĢäļ│┤Ļ│Āņ×É ĒĢ£ļŗż.
ļ│ĖļĪĀ
MS ļ│æļ│ĆņØś ņĀĢņØś(definition of MS lesion)
MRIņŚÉņä£ņØś MS ļ│æļ│ĆņØĆ T2, T2-fluid-attenuated inversion recovery (T2-FLAIR), proton density (PD)ņÖĆ Ļ░ÖņØĆ T2Ļ░ĢņĪ░ņśüņāüņŚÉņä£ ņøÉĒśĢ(round) ļśÉļŖö ĒāĆņøÉĒśĢ(ovoid)ņØś Ļ│ĀņŗĀĒśĖĻ░ĢļÅäļź╝ Ļ░Ćļ”¼Ēé©ļŗż. ļ╣äĒŖ╣ņØ┤ņĀüņØĖ T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäņÖĆ ĻĄ¼ļ│äĒĢśĻĖ░ ņ£äĒĢ┤ MS ļ│æļ│ĆņØĆ ņןņČĢ(long axis) ņ¦Ćļ”äņØ┤ ņĄ£ņåī 3 mm ņØ┤ņāüņØ┤ņ¢┤ņĢ╝ ĒĢ£ļŗż. Ļ▓ĮņÜ░ņŚÉ ļö░ļØ╝ņä£ 1-2 cm ņØ┤ņāü Ēü┤ ņłśļÅä ņ׳ļŗż. MRI ĒŚłņāü(artifact)ņŚÉ ņØśĒĢ£ T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅä Ļ░ĆļŖźņä▒ņØä ļ░░ņĀ£ĒĢśĻĖ░ ņ£äĒĢ┤ ņä£ļĪ£ ļŗżļźĖ ņŗ£ĒĆĆņŖż, ņśłļź╝ ļōżņ¢┤ T2ņÖĆ T2-FLAIR ļśÉļŖö T2ņÖĆ PD Ļ░ĢņĪ░ņśüņāüņØś Ļ░ÖņØĆ ņ£äņ╣śņŚÉņä£ ļÅÖņŗ£ņŚÉ Ļ│ĀņŗĀĒśĖĻ░ĢļÅäĻ░Ć ļ│┤ņŚ¼ņĢ╝ ĒĢ£ļŗż. ļśÉĒĢ£ T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäĻ░Ć Ļ░ĆĻĖēņĀü 2Ļ░£ ņØ┤ņāü ņŚ░ņåŹļÉ£ ņĀłĒÄĖ(slice)ņŚÉņä£ ļ│┤ņŚ¼ņĢ╝ MS ļ│æļ│Ćņ£╝ļĪ£ Ļ░äņŻ╝ĒĢśļÅäļĪØ ĻČīĻ│ĀĒĢśņ¦Ćļ¦ī MRI ņśüņāüņØä 3 mm ņĀłĒÄĖļæÉĻ╗ś(slice thickness)ļ│┤ļŗż ļæÉĻ╗ŹĻ▓ī ĒÜŹļōØĒĢśņśĆņØä Ļ▓ĮņÜ░ņŚÉļŖö 1Ļ░£ ņĀłĒÄĖņŚÉņä£ļ¦ī ļ│┤ņØ╝ ņłśļÅä ņ׳ņØīņØä Ļ░ÉņĢłĒĢ┤ņĢ╝ ĒĢ£ļŗż.
MS ļ│æļ│ĆņØĆ ņżæņČöņŗĀĻ▓ĮĻ│ä ļé┤ ņ¢┤ļööļōĀņ¦Ć ļ░£ņāØĒĢĀ ņłś ņ׳ļŗż. ĻĘĖļ¤¼ļéś ņżæņČöņŗĀĻ▓ĮĻ│äļź╝ ņ╣©ļ▓öĒĢśļŖö ņ£Āņé¼ņ¦łĒÖśĻ│╝ ļŗ¼ļ”¼ ĒŖ╣ņĀĢ ņ£äņ╣śņŚÉ ļ│æļ│ĆņØ┤ ĒśĖļ░£ĒĢśļŖö ļÅģĒŖ╣ĒĢ£ ĒŖ╣ņä▒ņØ┤ ņ׳ļŗż. ņśłļź╝ ļōżņ¢┤ ļćīņŗżņŻ╝ņ£äļ░▒ņ¦ł(periventricular white matter, PVWM), Ēö╝ņ¦łĻ│üļ░▒ņ¦ł(juxtacortical white matter) ļśÉļŖö Ēö╝ņ¦ł(cortical), ļćīļ¤ē(corpus callosum), ļŗżļ”¼ļćīņÖĆ ņåīļćī Ļ░ÖņØĆ ņ▓£ļ¦ēĒĢś(infratentorial) ĻĄ¼ņĪ░ļ¼╝, Ļ▓ĮņČöļČĆ ņ▓Öņłś(cervical spinal cord) ļō▒ņØ┤ ĒśĖļ░£ ļČĆņ£äņØ┤ļ®░, ņØ┤ļ¤¼ĒĢ£ ĒŖ╣ņĀĢ ņ£äņ╣śĻ░Ć McDonald ņ¦äļŗ© ĻĖ░ņżĆņØś MRI DISņŚÉ ļ░śņśüļÉśņ¢┤ ņ׳ļŗż. McDonald ņ¦äļŗ© ĻĖ░ņżĆņØś MRI DIS ĻĖ░ņżĆņØä ļ¦īņĪ▒ĒĢśļĀżļ®┤ 1) ļćīņŗżņŻ╝ņ£äļ░▒ņ¦ł, 2) Ēö╝ņ¦łĻ│üļ░▒ņ¦ł ļśÉļŖö Ēö╝ņ¦ł, 3) ņ▓£ļ¦ēĒĢś, 4) ņ▓Öņłś 4Ļ░£ņØś ņżæņČöņŗĀĻ▓ĮĻ│ä ņśüņŚŁ ņżæ ņĄ£ņåī 2Ļ░£ ņØ┤ņāüņØś ņśüņŚŁņŚÉņä£ MS ņĀäĒśĢņĀüņØĖ T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäĻ░Ć ļ│┤ņŚ¼ņĢ╝ ĒĢ£ļŗż. ļŗżņØīņŚÉņä£ DIS ĻĖ░ņżĆņŚÉ ļīĆĒĢ┤ ņ×ÉņäĖĒ׳ ņé┤ĒÄ┤ļ│┤ļÅäļĪØ ĒĢśĻ▓Āļŗż.
Ļ│ĄĻ░äņĀü Ēīīņóģ(DIS) ĻĖ░ņżĆ
ļćīņŗżņŻ╝ņ£äļ░▒ņ¦ł(PVWM)
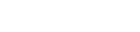
ļćīņŗżņŻ╝ņ£äļ░▒ņ¦ł(PVWM) ļ│æļ│ĆņØĆ Ļ░Ćņ¬Įļćīņŗż(lateral ventricle)Ļ│╝ ņ¦üņĀæņĀüņ£╝ļĪ£ ļ¦×ļŗ┐ņĢä ņ׳ļŖö T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäļĪ£ ņĀĢņØśĒĢ£ļŗż. ļ│æļ│ĆĻ│╝ Ļ░Ćņ¬Įļćīņŗż ņé¼ņØ┤ņŚÉ ņĀĢņāü ļ░▒ņ¦łņØ┤ ļü╝ņ¢┤ļōżņ¢┤ ņ׳ņ£╝ļ®┤ ņĢł ļÉ£ļŗż(Fig. 1A). Ļ░Ćņ¬ĮļćīņŗżĻ│╝ ņ¦üņĀæ ļ¦×ļŗ┐ņĢä ņ׳ļŖö ļćīļ¤ēņØś T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäļÅä ļćīņŗżņŻ╝ņ£äļ░▒ņ¦ł ļ│æļ│Ćņ£╝ļĪ£ ĒżĒĢ©ļÉĀ ņłś ņ׳ļŗż. ĒĢśņ¦Ćļ¦ī T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäĻ░Ć Ļ░Ćņ¬ĮļćīņŗżĻ│╝ ņ¦üņĀæ ļ¦×ļŗ┐ņĢä ņ׳ļŹöļØ╝ļÅä Ļ╝¼ļ”¼ĒĢĄ(caudate nucleus)ņØ┤ļéś ņŗ£ņāü(thalamus)Ļ│╝ Ļ░ÖņØĆ ņŗ¼ļČĆĒÜīņāēņ¦łņŚÉ ņ£äņ╣śĒĢ£ļŗżļ®┤ ļćīņŗżņŻ╝ņ£äļ░▒ņ¦ł ļ│æļ│Ćņ£╝ļĪ£ ĒżĒĢ©ņŗ£Ēéżņ¦Ć ņĢŖļŖöļŗż.10 ļśÉĒĢ£ ņĀ£3, 4ļćīņŗżņŚÉ ņ¦üņĀæ ļ¦×ļŗ┐ņĢä ņ׳ļŖö T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäļÅä ļćīņŗżņŻ╝ņ£äļ░▒ņ¦ł ļ│æļ│Ćņ£╝ļĪ£ ĒżĒĢ©ņŗ£Ēéżņ¦Ć ņĢŖļŖöļŗż. McDonald ņ¦äļŗ© ĻĖ░ņżĆņØś ŌĆśļćīņŗżņŻ╝ņ£äŌĆÖļŖö Ļ░Ćņ¬ĮļćīņŗżņØä ņ¦Ćņ╣ŁĒĢśļ®░ ņĀ£3, 4ļćīņŗż ļ░Å ņłśļÅäĻ┤ĆņŻ╝ņ£äļŖö ņĀ£ņÖĖĒĢ£ļŗż.
ĒŖ╣Ē׳ MSņŚÉņä£ņØś ļćīņŗżņŻ╝ņ£äļ░▒ņ¦ł ļ│æļ│ĆņØĆ ĒāĆņøÉĒśĢ T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäņØś ņןņČĢņØ┤ Ļ░Ćņ¬ĮļćīņŗżņŚÉ ļīĆĒĢśņŚ¼ ņłśņ¦ü ļ░®Ē¢ź(perpendicular) ļ░░ņŚ┤ņØä ļ│┤ņØ┤ļŖö ĒŖ╣ņ¦ĢņØä Ļ░¢ļŖöļŹ░ ņØ┤ļź╝ DawsonŌĆÖs fingerļØ╝Ļ│Ā ņ¦Ćņ╣ŁĒĢśļ®░(Fig. 1B) Ļ░Ćņ¬Įļćīņŗż ĻĘ╝ņ▓śņŚÉ ļ░▒ņ¦ł ļ│æļ│ĆņØä ļ│┤ņØ╝ ņłś ņ׳ļŖö MS ņ£Āņé¼ņ¦łĒÖśĻ│╝ņØś ņżæņÜöĒĢ£ ĻĄ¼ļ│äņĀÉņØ┤ ļÉ£ļŗż. ļ│æļ│ĆņØś ņØ┤ļ¤¼ĒĢ£ Ļ│ĄĻ░äņĀü ļ░░ņŚ┤(topographic)ņØĆ ļ│æļ”¼ņĀüņ£╝ļĪ£ ņŗ¼ļČĆņłśņ¦łņĀĢļ¦ź(deep medullary vein) ņŻ╝ļ│ĆļČĆņŚÉ ņŚ╝ņ”Ø, ļ”╝ĒöäĻĄ¼ ņ╣©ņ£żĻ│╝ ĒÖ£ļÅÖņä▒ MSĒīÉ(active MS plaque)ņØä ļ│┤ņØ┤ļŖö MS ĒŖ╣ņ¦ĢĻ│╝ ņØ╝ņ╣śĒĢ£ļŗż11. ņĀĢņāü ļģĖĒÖöņŚÉņä£ ļ│┤ņØ╝ ņłś ņ׳ļŖö Ļ░Ćņ¬Įļćīņŗż ļ┐ö(horn of lateral ventricle)ņØś cappingņØ┤ļéś(Fig. 2A) ĒÄĖļæÉĒåĄ, ĒŚłĒśłņä▒ ņåīĒśłĻ┤Ćņ¦łĒÖśņŚÉņä£ ļ│┤ņØ╝ ņłś ņ׳ļŖö T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅä(Fig. 2B)ļź╝ ļćīņŗżņŻ╝ņ£äļ░▒ņ¦ł ļ│æļ│Ćņ£╝ļĪ£ ņלļ¬╗ ļČäļźśĒĢĀ ņłś ņ׳ņ¢┤ ņŻ╝ņØśĻ░Ć ĒĢäņÜöĒĢśļŗż.12,13 ļćīļ¤ēņØĆ MSĻ░Ć ņĢäļŗī ļŗżļźĖ ņżæņČöņŗĀĻ▓ĮĻ│ä ņŚ╝ņ”Øņä▒ Ēāłņłśņ┤łņ¦łĒÖśņŚÉņä£ļÅä ļ│æļ│ĆņØ┤ ņēĮĻ▓ī Ļ┤Ćņ░░ļÉśļŖö Ļ││ņØ┤ļŗż. Susac ņ”ØĒøäĻĄ░ņØĆ MSņÖĆ ņ£Āņé¼ĒĢ£ ļćīļ¤ē ļ│æļ│ĆņØ┤ ļ│┤ņØ╝ ņłś ņ׳ļŖö ļō£ļ¼Ė ņ×ÉĻ░Ćļ®┤ņŚŁņä▒ ļ»ĖņäĖĒśłĻ┤Ćļ│æņ”Øņ£╝ļĪ£ ļŗżņØīĻ│╝ Ļ░ÖņØĆ ĒśĢĒā£ņØś ļćīļ¤ē ļ│æļ│ĆņØ┤ ļ│┤ņØ╝ ņłś ņ׳ļŖöļŹ░ ņøÉĒśĢņØś T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäĻ░Ć ļćīļ¤ē ņżæņŗ¼ņä¼ņ£Ā(central fiber), ņ”ē Ļ░Ćņ¬ĮļćīņŗżĻ│╝ ļćīļ¤ē ņ▓£ņן(roof, superior surface) ņé¼ņØ┤ņŚÉ ņ£äņ╣śĒĢ£ snowball ĒśĢĒā£, ļćīļ¤ē ņ▓£ņןņ£╝ļĪ£ļČĆĒä░ ņĢäļל ļ░®Ē¢źņ£╝ļĪ£ Ē¢źĒĢśļŖö ņé╝Ļ░üĒśĢ Ļ│Āļō£ļ”ä ļ¬©ņ¢æņØś icicle ĒśĢĒā£, ļćīļ¤ē ņ▓£ņןņŚÉ ņłśņ¦ü ļ░®Ē¢źņ£╝ļĪ£ ļéśĒāĆļéśļŖö ļČĆņ▒äņé┤ ļ¬©ņ¢æņØś spoke ĒśĢĒā£ ļō▒ņØĆ Susac ņ”ØĒøäĻĄ░ņØä ņŗ£ņé¼ĒĢśļŖö ĒŖ╣ņ¦ĢņĀüņØĖ ļ¬©ņ¢æņØ┤ļŗż.14,15 ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ļ▓öņŻ╝ņ¦łĒÖś(neuromyelitis optica spectrum disorder, NMOSD)ņØĆ ļØ╝Ēŗ┤ņĢäļ®öļ”¼ņ╣┤ņØĖ, ĒØæņØĖ, ņĢäņŗ£ņĢäņØĖņŚÉņä£ MSļ│┤ļŗż ņāüļīĆņĀüņ£╝ļĪ£ ļ░£ņāØļźĀņØ┤ ļåÆĻĖ░ ļĢīļ¼ĖņŚÉ Ļ╝Ł ļ░░ņĀ£ĒĢ┤ņĢ╝ ĒĢśļŖö ņ¦łĒÖśņØ┤ļ®░ NMOSDņŚÉņä£ņØś ļćīļ¤ē ļ│æļ│ĆņØĆ ļČłļČäļ¬ģĒĢ£ Ļ▓ĮĻ│ä(blurred margin), ļ│æļ│Ć ņŻ╝ļ│ĆļČĆ T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäņÖĆ ņżæņŗ¼ļČĆ T2 ņĀĆņŗĀĒśĖĻ░ĢļÅäļź╝ ņØ┤ņ¦łņĀüņ£╝ļĪ£ ļ│┤ņØ┤ļŖö marbled ĒśĢĒā£, ļćīļ¤ē ĒŖ╣Ē׳ ĒīĮļīĆļČĆņ£ä(splenium) ņĀäņ▓┤ņŚÉ ļæÉĻ║╝ņÜ┤ T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäļź╝ ļ│┤ņØ┤ļŖö arch-bridge ĒśĢĒā£, ļ│æļ│Ć Ļ░Ćņןņ×Éļ”¼Ļ░Ć ĒØÉļ”┐ĒĢśļ®┤ņä£ ļŗżļ░£ ļ░śņĀÉĒśĢ(multiple patchy) ņĪ░ņśüņ”ØĻ░ĢņØä ļ│┤ņØ┤ļŖö cloud-like enhancement ĒśĢĒā£Ļ░Ć ĒŖ╣ņ¦ĢņĀüņØ┤ļŗż.16,17 ņĢ×ņä£ ņ¢ĖĻĖēĒĢ£ ļćīļ¤ē ļ│æļ│ĆņØä ļ│┤ņØ╝ Ļ▓ĮņÜ░ MSĻ░Ć ņĢäļŗÉ Ļ░ĆļŖźņä▒ņØ┤ ļåÆņ£╝ļ®░ ļćīņŗżņŻ╝ņ£äļ░▒ņ¦ł ļ│æļ│Ćņ£╝ļĪ£ ļČäļźśĒĢ┤ņä£ļÅä ņĢł ļÉ£ļŗż.
Ēö╝ņ¦łĻ│üļ░▒ņ¦ł ļśÉļŖö Ēö╝ņ¦ł ļ│æļ│Ć(juxtacortical JC or cortical lesion)
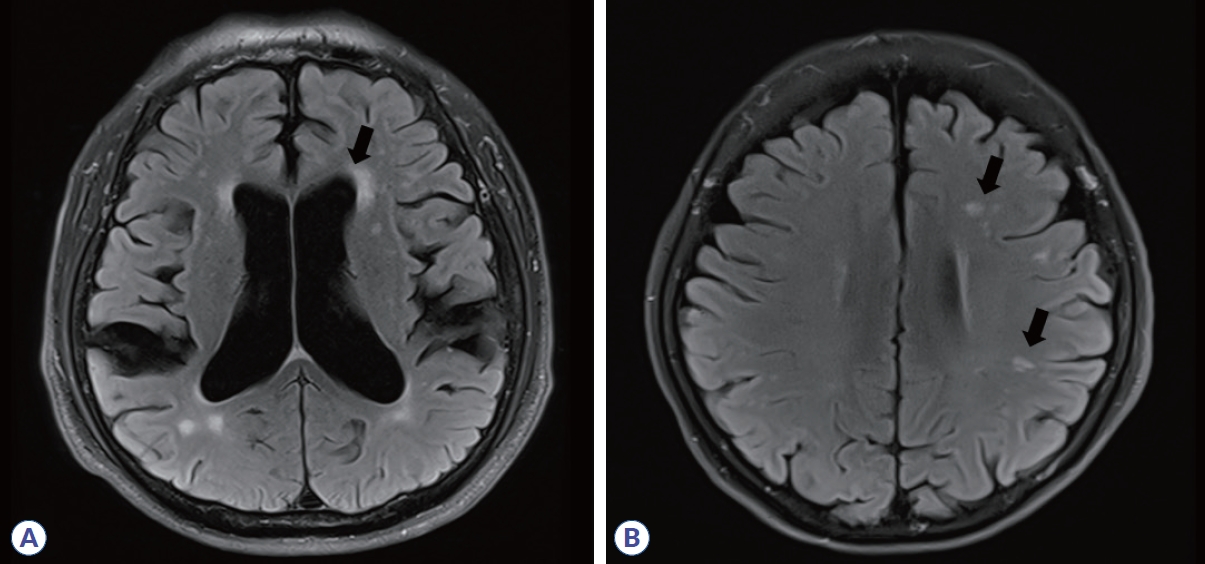
Ēö╝ņ¦łĻ│üļ░▒ņ¦ł(JC) ļ│æļ│ĆņØĆ ņĀĢņāü ļ░▒ņ¦łņØś ļü╝ņ¢┤ļō” ņŚåņØ┤ Ēö╝ņ¦łņŚÉ ņ¦üņĀæņĀüņ£╝ļĪ£ ļ¦×ļŗ┐ņĢä ņ׳ļŖö T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäļĪ£ ņĀĢņØśĒĢ£ļŗż. T2-FLAIR ņŗ£ĒĆĆņŖżņŚÉņä£ Ļ░Ćņן ļ░£Ļ▓¼ĒĢśĻĖ░ ņēĮļŗż. MSņØś Ēö╝ņ¦łĻ│üļ░▒ņ¦ł ļ│æļ│ĆņØĆ ĒØöĒ׳ Ēö╝ņ¦łĒĢś Uņä¼ņ£Ā(subcortical U-fiber)ļź╝ ņ╣©ļ▓öĒĢśļ®░(Fig. 3A), ļ░śļ®┤ ĒÄĖļæÉĒåĄņØ┤ļéś ĒŚłĒśłņä▒ ņåīĒśłĻ┤Ćņ¦łĒÖśņØĆ Ēö╝ņ¦ł ĻĘ╝ņ▓ś ļ░▒ņ¦łņŚÉ ļ│æļ│ĆņØ┤ ņ׳ļŹöļØ╝ļÅä Uņä¼ņ£ĀļŖö ņ╣©ļ▓öĒĢśņ¦Ć ņĢŖņĢä MSņÖĆ Ļ░Éļ│äņĀÉņØ┤ ļÉ£ļŗż.
Ēö╝ņ¦ł ļ│æļ│ĆņØĆ ņĪ░ņ¦üĒĢÖņĀü ņåīĻ▓¼ņŚÉ ļö░ļØ╝ 4Ļ░Ćņ¦Ć ņ£ĀĒśĢ ņ”ē, (1) type 1 leukocortical (MSĒīÉņØ┤ Ēö╝ņ¦łļČĆĒä░ Uņä¼ņ£Āļź╝ ĒżĒĢ©ĒĢ£ Ēö╝ņ¦łĻ│üļ░▒ņ¦łĻ╣īņ¦Ć ļ¬©ļæÉ ņ╣©ļ▓öĒĢ£ Ļ▓ĮņÜ░), (2) type 2 intracortical (MSĒīÉņØ┤ ņŚ░ņ¦łļ¦ēĻ│╝ Ēö╝ņ¦łĻ│üļ░▒ņ¦ł ļ¬©ļæÉ ņØĖņĀæĒĢśņ¦Ć ņĢŖĻ│Ā ņł£ņłśĒĢśĻ▓ī Ēö╝ņ¦ł ļé┤ņŚÉņä£ļ¦ī ņ׳ļŖö Ļ▓ĮņÜ░), (3) type 3 subpial demyelination (MSĒīÉņØ┤ ņŚ░ņ¦łļ¦ēļČĆĒä░ ņŗ£ņ×æĒĢśņŚ¼ Ēö╝ņ¦ł ļé┤ņŚÉ ņ׳ļŖö Ļ▓ĮņÜ░), (4) type 4 (MSĒīÉņØ┤ Ēö╝ņ¦ł ņĀäņ▓┤ņŚÉ Ļ▒Ėņ│É ņ׳ņ¦Ćļ¦ī Ēö╝ņ¦łĻ│üļ░▒ņ¦łņØĆ ņ╣©ļ▓öĒĢśņ¦Ć ņĢŖņØĆ Ļ▓ĮņÜ░)ļĪ£ ļČäļźśĒĢ£ļŗż18. T2-FLAIR ņŗ£ĒĆĆņŖżņŚÉņä£ ņŻ╝ļĪ£ Ļ┤Ćņ░░ĒĢĀ ņłś ņ׳ņ¦Ćļ¦ī double inversion recovery, phase-sensitive inversion recovery Ļ░ÖņØĆ ĒŖ╣ņłś MRIļź╝ ņØ┤ņÜ®ĒĢĀ Ļ▓ĮņÜ░ ļŹö ņל ļ│╝ ņłś ņ׳ņ£╝ļ®░ Ļ│ĪņäĀ ĒśĢĒā£(curvilinear)ņØś Ēö╝ņ¦ł ļ│æļ│ĆņØĆ ĒŖ╣Ē׳ MS ĒŖ╣ņØ┤ņĀüņØ┤ļŗż(Fig. 3B).19 ĻĘĖļ¤¼ļéś ĒŚłņāüņØä Ēö╝ņ¦ł ļ│æļ│Ćņ£╝ļĪ£ ņ░®ņśżĒĢĀ Ļ░ĆļŖźņä▒ņØ┤ ļåÆĻĖ░ ļĢīļ¼ĖņŚÉ ņŻ╝ņØśņÖĆ ĒøłļĀ©ņØ┤ ĒĢäņÜöĒĢśļŗż. ņŗżņĀ£ ņ¦äļŻīĒśäņןņŚÉņä£ ņŻ╝ļĪ£ ņé¼ņÜ®ĒĢśļŖö 1.5 ļśÉļŖö 3.0 ĒģīņŖ¼ļØ╝ MRIļĪ£ļŖö Ēö╝ņ¦ł ļ│æļ│ĆņØä ĒāĆņ×ģļ│äļĪ£ ļ¬ģļŻīĒĢśĻ▓ī ĻĄ¼ļČäĒĢśĻĖ░ļŖö ņ¢┤ļĀĄĻĖ░ ļĢīļ¼ĖņŚÉ leukocortical, intracortical, JC ļ¬©ļæÉ Ēö╝ņ¦łĻ│üļ░▒ņ¦ł ļ│æļ│Ćņ£╝ļĪ£ ņĢäņÜĖļ¤¼ ņāØĻ░üĒĢśĻĖ░ļĪ£ ĒĢśņśĆļŗż.20
ņ▓£ļ¦ēĒĢś ļ│æļ│Ć(infratentorial lesion)
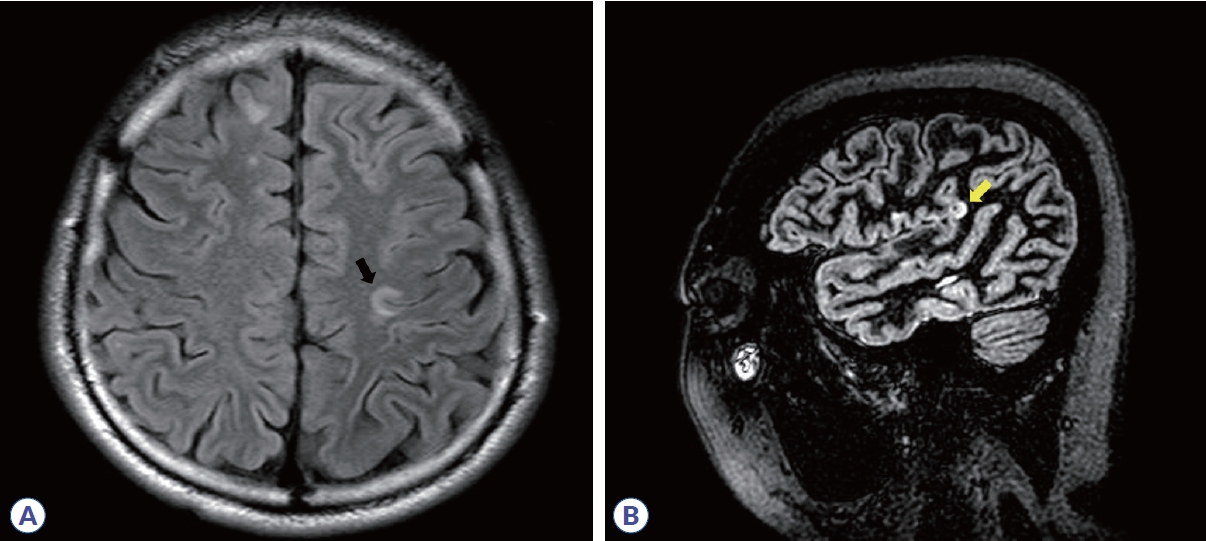
ņ▓£ļ¦ēĒĢś ļ│æļ│ĆņØĆ ļćīņżäĻĖ░, ņåīļćīļŗżļ”¼(cerebellar peduncle), ņåīļćīņŚÉņä£ ļ│┤ņØ┤ļŖö T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäļĪ£ ņĀĢņØśĒĢ£ļŗż. ĒŖ╣Ē׳ ļŗżļ”¼ļćīņŚÉņä£ Ļ░Ćņן ņל Ļ┤Ćņ░░ļÉśļ®░ ņŻ╝ļ│ĆļČĆ(periphery) Ēæ£ļ®┤(surface)ņŚÉ ņ£äņ╣śĒĢśļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äļŗż. ņåīļćīļŗżļ”¼ļćīņłśņĪ░(cerebellopontine cistern)ļź╝ ĒżĒĢ©ĒĢ£ ņłśņĪ░(cistern) ņŻ╝ņ£äļéś ņĀ£4ļćīņŗż ĻĘ╝ņ▓ś, ņé╝ņ░©ņŗĀĻ▓Į ņ¦äņ×ģļČĆņ£ä(root entry zone of trigeminal nerve)ņ▓śļ¤╝ ņłśņ┤łĻ░Ć ĒÆŹļČĆĒĢśļ®┤ņä£ ļćīņ▓ÖņłśņĢĪĻ│╝ Ļ░ĆĻ╣īņÜ┤ Ļ││ņŚÉņä£ ļ│╝ ņłś ņ׳ļŗż(Fig. 4A). ņ▓£ļ¦ēĒĢś ļČĆņ£äļŖö MSĻ░Ć ņĢäļŗī ņŚ¼ļ¤¼ ņżæņČöņŗĀĻ▓ĮĻ│ä ņ¦łĒÖśņŚÉņä£ļÅä ļ│æļ│ĆņØ┤ ļ░£ņāØĒĢśļŖö ņ£äņ╣śņØ┤ĻĖ░ ļĢīļ¼ĖņŚÉ ļ░░ņĀ£ ņ¦äļŗ©ņØ┤ ņżæņÜöĒĢśļŗż. ĒŚłĒśłņä▒ ņåīĒśłĻ┤Ćņ¦łĒÖśņØĆ Ļ░üĻ░üņØś Ļ┤ĆĒåĄļÅÖļ¦źļōżņØ┤ Ēśłļźśļź╝ Ļ│ĄĻĖēļ░øĻĖ░ ļĢīļ¼ĖņŚÉ Ļ▓ĮĻ│äĻĄ¼ņŚŁ(border zone)ņØ┤ ļÉśĻĖ░ ņē¼ņÜ┤ ļŗżļ”¼ļćī ņżæņŗ¼ļČĆņŚÉņä£ ņŻ╝ļĪ£ T2 ņŗĀĒśĖ ļ│ĆĒÖöĻ░Ć ļ│┤ņØ┤ļ®░(Fig. 4B)13 NMOSDļŖö ļ¦żņÜ░ ĒŖ╣ņ¦ĢņĀüņ£╝ļĪ£ ļ¦©ņĢäļלĻĄ¼ņŚŁ(area postrema)ņØ┤ļéś ņłśļÅäĻ┤ĆņŻ╝ņ£ä(periaqueductal)ņŚÉņä£ T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäļź╝ ļ│┤ņØĖļŗż(Fig. 4C).16 ļćīņżäĻĖ░ļéś ņåīļćīļŗżļ”¼ņŚÉ ļ│æļ│ĆņØ┤ ņ׳ļÉś ĒśĢĒā£Ļ░Ć ņå£ĒäĖ(fluffy)ņØ┤ļéś ĻĄ¼ļ”äņ▓śļ¤╝ ĒŹ╝ņ¦ä(fuzzy) Ļ▓ĮĻ│äņØ┤Ļ▒░ļéś ņ¢æņĖĪņä▒ņØ┤Ļ▒░ļéś ļ│æļ│Ć Ēü¼ĻĖ░Ļ░Ć ņłś cm ņØ┤ņāüņ£╝ļĪ£ Ēü┤ Ļ▓ĮņÜ░ ĒĢŁļ¦ÉņØ┤ņ¦æĒؼņåīļÅīĻĖ░ņĢäĻĄÉņäĖĒżļŗ╣ļŗ©ļ░▒ņ¦łĒĢŁņ▓┤Ļ┤ĆļĀ©ņ¦łĒÖś(myelin oligodendrocyte glycoprotein antibody-associated disease, MOGAD)21 (Fig. 4D)ņØ┤ļéś ņŗĀĻ▓Įļ▓Āņ▓┤ĒŖĖļ│æ(neuro-behcet disease) Ļ░ĆļŖźņä▒ņØ┤ ņ׳ļŗż.22
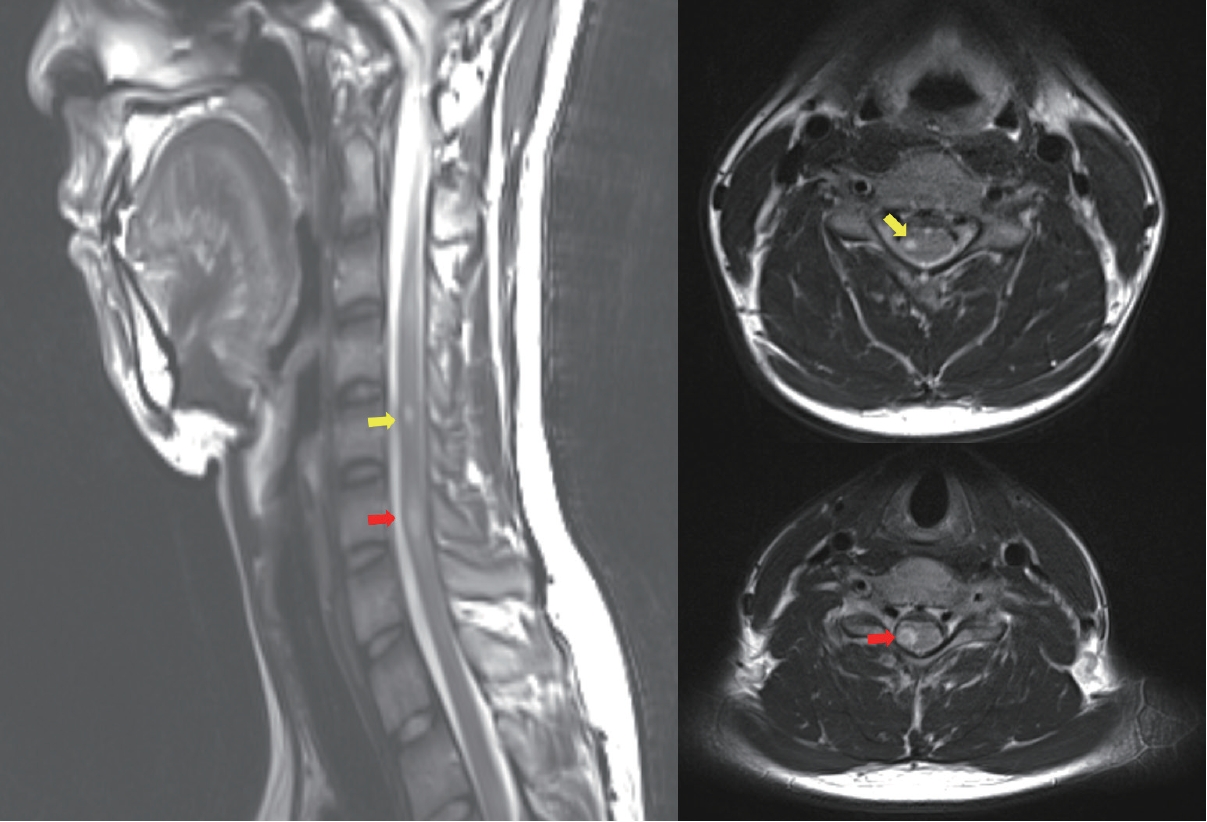
ņ▓Öņłś ļ│æļ│Ć(spinal cord lesion)
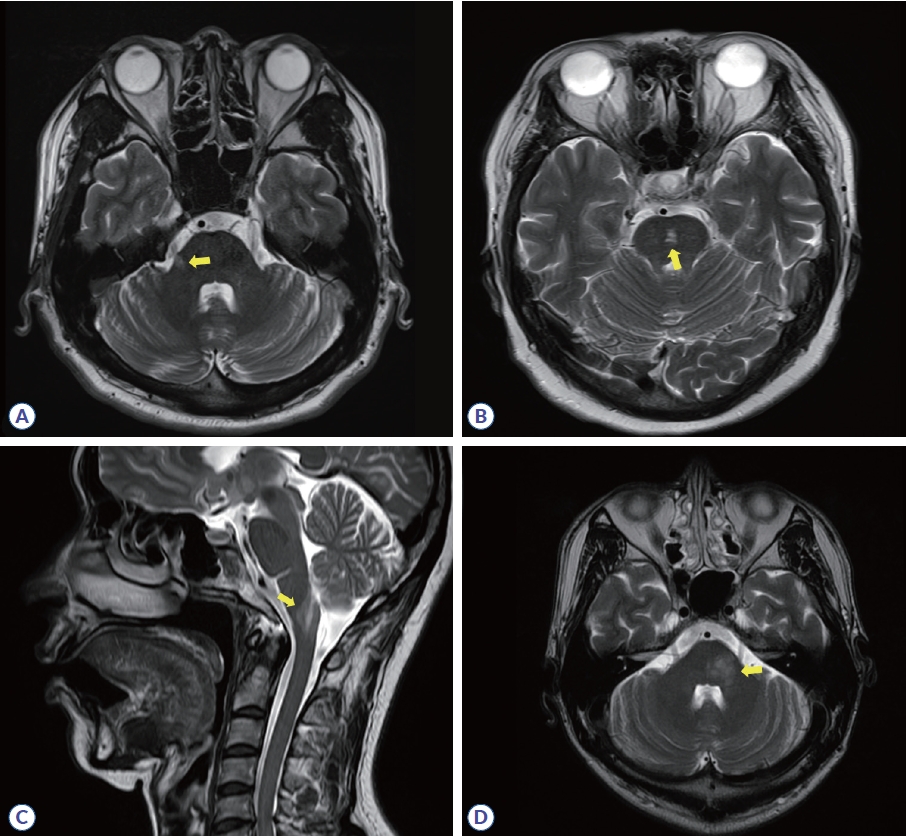
MSņŚÉņä£ņØś ņ▓Öņłś ļ│æļ│ĆņØĆ ļćīļé┤ ļ│æļ│ĆĻ│╝ ļ¦łņ░¼Ļ░Ćņ¦ĆļĪ£ ņøÉĒśĢ ļśÉļŖö ĒāĆņøÉĒśĢņØś Ļ▓ĮĻ│äĻ░Ć ļ╣äĻĄÉņĀü ļČäļ¬ģĒĢ£ T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅäļĪ£ ņĀĢņØśĒĢśļ®░ Ļ▓Įņłś ļśÉļŖö Ļ▓ĮĒØēņłś Ļ▓ĮĻ│äļČĆņ£äņŚÉņä£ ņ×ÉņŻ╝ ļ│┤ņØĖļŗż. MSĒīÉņØ╝ Ļ░ĆļŖźņä▒ņØä ņóĆ ļŹö ņŗ£ņé¼ĒĢśļŖö ļ│┤ņĪ░ņĀü ĒŖ╣ņ¦Ģņ£╝ļĪ£ļŖö (1) ņāüĒĢśņóīņÜ░ ņ¦Ćļ”äņØ┤ ņ×æņĢäņä£ ņ▓Öņłś ļŗ©ļ®┤ņĀüņØś 1/2 ņØ┤ĒĢś, ņ▓ÖņČöļČäņĀł 2Ļ░£ ņØ┤ĒĢś; (2) ņŗ£ņāüļ®┤ņŚÉņä£ ļŗ┤ļ░░ ļ¬©ņ¢æ(cigar-shaped)ņØ┤ļ®┤ņä£ ņČĢļ®┤(axial)ņŚÉņä£ ņøÉĒśĢ, ĒāĆņøÉĒśĢ, ļśÉļŖö ņÉÉĻĖ░ļ¬©ņ¢æ(wedge-shaped); (3) ņ▓Öņłś ņŻ╝ļ│ĆļČĆ(periphery), ĻĘĖņżæņŚÉņä£ļÅä Ļ░Ćņ¬ĮĻĖ░ļæź(lateral column)Ļ│╝ ļō▒ņ¬ĮĻĖ░ļæź(dorsal column)ņŚÉ ņ£äņ╣śĒĢśļŖö Ļ│ĄĻ░äņĀü ļ░░ņŚ┤ ĒŖ╣ņä▒ņØ┤ ņ׳ļŗż(Fig. 5).23,24 ņ▓ÖņČöļČäņĀł 3Ļ░£ ņØ┤ņāü ĻĖĖņØ┤ņØ┤Ļ▒░ļéś ņ▓Öņłś ļŗ©ļ®┤ņĀü 1/2 ņØ┤ņāü ņ¦Ćļ”äņØś Ļ┤æļ▓öņ£äĒĢ£ ļ│æļ│ĆņØ┤Ļ▒░ļéś ņ▓Öņłś ņżæņŗ¼ļČĆ ĒÜīņāēņ¦łņØä ņŻ╝ļĪ£ ņ╣©ļ▓öĒĢśļŖö ļ│æļ│Ć, ņŚ░ņłśļ¦ē(leptomeningeal) ņĪ░ņśüņ”ØĻ░ĢņØ┤ ļæÉļō£ļ¤¼ņ¦ä ļ│æļ│Ć, ņ▓Öņłś ļČĆĻĖ░(swelling)Ļ░Ć ņŗ¼ĒĢ£ ļ│æļ│Ć, ļō▒ņ¬ĮĻĖ░ļæź ņäĀĒāØņĀüņØĖ ļ¦żņÜ░ ĻĖ┤ ļ│æļ│Ć, ņ▓Öņłś ņøÉļ┐ö(conus medullaris)ņŚÉ ņŻ╝ļĪ£ ĻĄŁĒĢ£ĒĢ£ ļ│æļ│ĆņØĆ NMOSD, ņŗĀĻ▓Įņé¼ļź┤ņĮöņØ┤ļō£ņ”Ø(neurosarcoidosis), Ļ░ÉņŚ╝, ņ▓Öņłśņóģņ¢æ, ņśüņ¢æĻ▓░ĒĢŹ, MOGAD Ļ░ĆļŖźņä▒ņØä ļŹö ņŗ£ņé¼ĒĢ£ļŗż.24-26
ņŗ£Ļ░äņĀü Ēīīņóģ(DIT) ĻĖ░ņżĆ
Ļ░ĆļÅīļ”¼ļŖä(gadolinium) ņĪ░ņśüņ”ØĻ░ĢņØĆ ņŻ╝ļĪ£ ņāłļĪ£ ņāØĻĖ┤ ņŚ╝ņ”Øņä▒ Ēāłņłśņ┤ł ļ│æļ│ĆņŚÉņä£ Ļ┤Ćņ░░ļÉśļ®░ ļīĆĻ░£ 2-8ņŻ╝ ņØ┤ļé┤ļĪ£ ņ¦ĆņåŹ ĻĖ░Ļ░äņØ┤ ņ¦¦ĻĖ░ ļĢīļ¼ĖņŚÉ ņśżļלļÉ£ ļ│æļ│ĆĻ│╝ņØś ĻĄ¼ļČäņŚÉ ņÜ®ņØ┤ĒĢśĻ│Ā ņŗ£Ļ░äņĀü ĒīīņóģņØä ņ×ģņ”ØĒĢśļŖö ĻĘ╝Ļ▒░ļĪ£ ĒÖ£ņÜ®ļÉĀ ņłś ņ׳ļŗż.27 ņĪ░ņśüņ”ØĻ░Ģ ĒśĢĒā£ļŖö Ļ▓░ņĀł(nodular)ņØ┤ļéś Ļ│Āļ”¼(ring) ņĪ░ņśüņ”ØĻ░Ģ ļ¬©ļæÉ ļ│┤ņØ╝ ņłś ņ׳ļŗż. ĻĘĖļ¤¼ļéś ņĪ░ņśüņ”ØĻ░Ģ ĒśĢĒā£Ļ░Ć ļ¦żņÜ░ ļ»Ėļ¦īņä▒(diffuse)ņØ┤Ļ▒░ļéś, ņŚ░ņłśļ¦ē ņĪ░ņśüņ”ØĻ░ĢņØ┤ ņ׳Ļ▒░ļéś, ĻĄŁņåī Ēö╝ņ¦łņŚÉļ¦ī ņĪ░ņśüņ”ØĻ░ĢņØ┤ ļ│┤ņØ┤Ļ▒░ļéś, ļÅÖņØ╝ĒĢ£ ļ│æļ│ĆņØ┤ 3Ļ░£ņøö ņØ┤ņāü ņ¦ĆņåŹņĀüņ£╝ļĪ£ ņĪ░ņśüņ”ØĻ░ĢņØä ļ│┤ņØ┤Ļ▒░ļéś ļ¬©ļōĀ ļ│æļ│ĆņØ┤ ļÅÖņŗ£ņŚÉ ņĪ░ņśüņ”ØĻ░ĢņØä ļ│┤ņØĖļŗżļ®┤ MSĻ░Ć ņĢäļŗÉ Ļ░ĆļŖźņä▒ņØä Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢ£ļŗż.28,29 2010 McDonald ņ¦äļŗ© ĻĖ░ņżĆņØĆ ņä£ļĪ£ ļŗżļźĖ ļ¼┤ņ”Øņāü MRI ļ│æļ│ĆņØ┤ ņĪ░ņśüņ”ØĻ░ĢļÉśļŖö Ļ▓āĻ│╝ ņĪ░ņśüņ”ØĻ░ĢļÉśņ¦Ć ņĢŖļŖö Ļ▓āņØ┤ ļÅÖņŗ£ņŚÉ ņ׳ņØä ļĢī DITļź╝ ļ¦īņĪ▒ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│Ā ņ”Øņāü ņ£Āļ░£ ļ│æļ│ĆņØĆ DIT ĒīÉļŗ© ņŗ£ ņĀ£ņÖĖĒĢśļÅäļĪØ ĒĢśņśĆņ£╝ļéś 2017 ņ¦äļŗ© ĻĖ░ņżĆļČĆĒä░ļŖö ņ”Øņāü ņ£Āļ░£ ļ│æļ│ĆņØś ņĪ░ņśüņ”ØĻ░ĢļÅä ļ¼┤ņ”Øņāü ļ│æļ│ĆĻ│╝ ļÅÖņØ╝ĒĢśĻ▓ī DIT ĻĖ░ņżĆņŚÉ ĒżĒĢ©ļÉśļÅäļĪØ Ļ░£ņĀĢļÉśņŚłļŗż.
ņāłļĪŁĻ▓ī ļČĆĻ░üļÉśļŖö MS ĒŖ╣ņØ┤ņĀü ņåīĻ▓¼(emerging MS-specific MRI features)
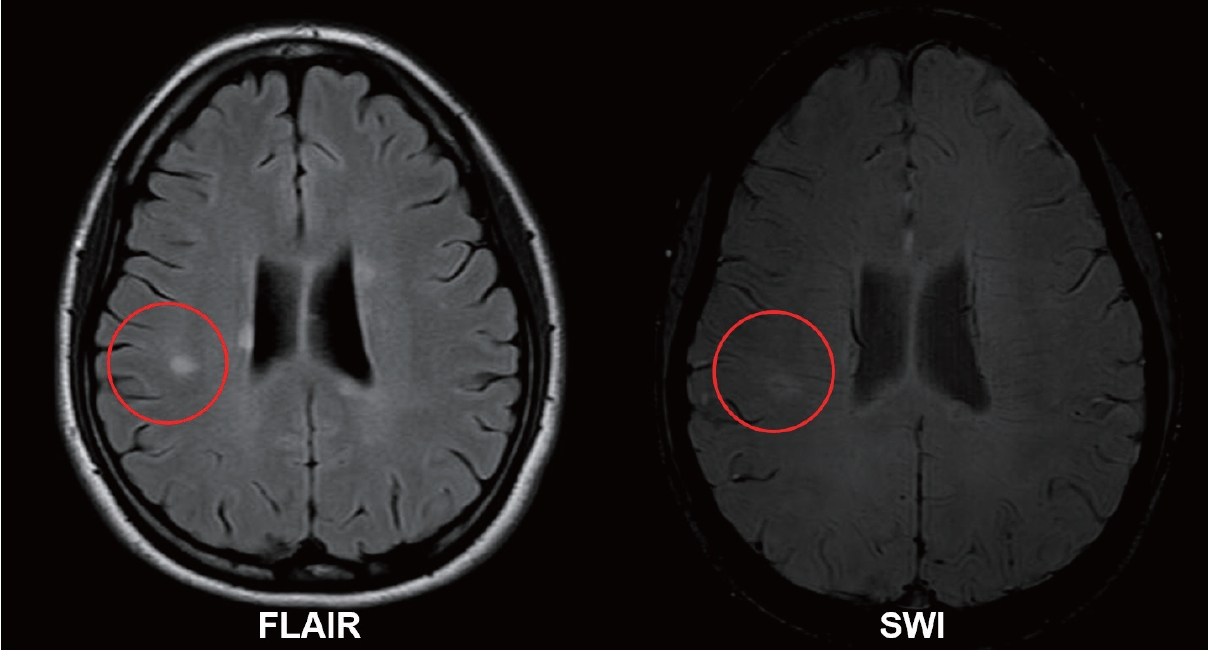
ņżæņŗ¼ņĀĢļ¦źņŗĀĒśĖ(central vein sign, CVS)
ņĢ×ņä£ ņ¢ĖĻĖēĒĢ£ Ļ▓āņ▓śļ¤╝ MSĒīÉņØĆ ņĪ░ņ¦üĒĢÖņĀüņ£╝ļĪ£ ņŗ¼ļČĆņłśņ¦łņĀĢļ¦ź ņŻ╝ļ│ĆļČĆņŚÉ ņל ļ░£ņāØĒĢśļŖö ĒŖ╣ņ¦ĢņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ļŖöļŹ░ MR ņ┤¼ņśüĻĖ░ņłĀņØ┤ ļ░£ņĀäĒĢ©ņŚÉ ļö░ļØ╝ ņśüņāüņ£╝ļĪ£ MSĒīÉĻ│╝ ĒīÉņØä Ļ┤ĆĒåĄĒĢśļŖö ņŗ¼ļČĆņżæņŗ¼ņĀĢļ¦ź(central vein and venule)ņØä ņŗ£Ļ░üĒÖöĒĢĀ ņłś ņ׳Ļ▓ī ļÉśņŚłĻ│Ā ņØ┤ļź╝ ņżæņŗ¼ņĀĢļ¦źņŗĀĒśĖ(CVS)ļØ╝Ļ│Ā ļ¬ģļ¬ģĒĢśņśĆļŗż. T2*Ļ░ĢņĪ░ņśüņāü(ĒŖ╣Ē׳ T2* weighted segmented echo-planar imaging)Ļ│╝ FLAIR*ņśüņāüņŚÉņä£ ņל Ļ┤Ćņ░░ļÉśļ®░ ņ×ÉĒÖöņ£©Ļ░ĢņĪ░ņśüņāüņŚÉņä£ļÅä Ļ┤Ćņ░░ĒĢĀ ņłś ņ׳ņ£╝ļéś ņĀäņłĀĒĢ£ ņśüņāüļ│┤ļŗżļŖö CVS Ļ▓ĆņČ£ņŚÉ ņ׳ņ¢┤ ņĢĮĻ░ä ņŚ┤ļō▒ĒĢśļŗż. ņØ┤ļ¤¼ĒĢ£ ņ┤¼ņśüĻĖ░ņłĀļōżņØĆ ļ░▒ņ¦ł ļ│æļ│Ć ļé┤ņØś CVS Ļ▓ĆņČ£ņŚÉ ņśłļ»╝ĒĢśĻĖ░ ļĢīļ¼ĖņŚÉ MSņÖĆ ļ╣äMS ļ│æļ│Ć Ļ░Éļ│äņØä ņ£äĒĢ£ ņŚ░ĻĄ¼ņŚÉ ļ¦ÄņØ┤ ĒÖ£ņÜ®ļÉśņŚłĻ│Ā CVS ņ£Āļ¼┤Ļ░Ć MSņŚÉ ļ¦żņÜ░ ĒŖ╣ņØ┤ņĀüņØ┤ļØ╝ļŖö ļ│┤Ļ│ĀļōżņØ┤ ļłäņĀüļÉśĻ│Ā ņ׳ļŗż.30-32 CVSļŖö 2 mm ļ»Ėļ¦ī ņ¦üĻ▓ĮņØś Ļ░ĆļŖö ņäĀ(line) ļśÉļŖö ņĀÉ(dot) ļ¬©ņ¢æ ņĀĆņŗĀĒśĖĻ░ĢļÅäļĪ£, ņĀäĒśĢņĀüņØĖ MSĒīÉ(ņןņČĢ 3 mm ņØ┤ņāüņØś ņøÉĒśĢ ļśÉļŖö ĒāĆņøÉĒśĢņØś T2 Ļ│ĀņŗĀĒśĖĻ░ĢļÅä ļ│æļ│Ć) ĒĢ£ Ļ░ĆņÜ┤ļŹ░ļź╝ Ļ░ĆļĪ£ņ¦Ćļź┤ļŖö ļ│æļ│Ćņ£╝ļĪ£ ņĀĢņØśĒĢ£ļŗż(Fig. 6). MS ļ░▒ņ¦ł ļ│æļ│ĆņŚÉņä£ļŖö 1Ļ░£ņØś CVSļ¦ī Ļ┤Ćņ░░ļÉśļ®░ ļ¦īņĢĮ ņŚ¼ļ¤¼ Ļ░£ņØś ņĀĢļ¦źņŗĀĒśĖĻ░Ć ļ│┤ņØ┤ļ®┤ CVSļĪ£ Ļ░äņŻ╝ĒĢśņ¦Ć ņĢŖļŖöļŗż. MSļź╝ Ļ░ĢĒĢśĻ▓ī ņŗ£ņé¼ĒĢśļŖö CVS Ļ┤ĆļĀ© ĻĖ░ņżĆņØĆ ņŚ¼ļ¤¼ Ļ░Ćņ¦ĆĻ░Ć ņĀ£ņŗ£ļÉśņ¢┤ ņÖöļŖöļŹ░ (1) ņĀäņ▓┤ ļ░▒ņ¦ł ļ│æļ│ĆņØś 40% ņØ┤ņāüņŚÉņä£ CVSĻ░Ć Ļ┤Ćņ░░ļÉśļŖö Ļ▓ā, (2) ņĀäĒśĢņĀüņØĖ CVSĻ░Ć 6Ļ░£ ņØ┤ņāü Ļ┤Ćņ░░ļÉśļŖö Ļ▓ā, (3) ļ¦īņĢĮ ļ░▒ņ¦ł ļ│æļ│Ć ņ┤Ø Ļ░£ņłśĻ░Ć 6Ļ░£ ņØ┤ĒĢśļØ╝ļ®┤ ļ¬©ļōĀ ļ│æļ│ĆņŚÉņä£ CVSĻ░Ć ļ│┤ņŚ¼ņĢ╝ ĒĢśļŖö Ļ▓ā, (4) ņĀäĒśĢņĀüņØĖ CVSĻ░Ć 3Ļ░£ ņØ┤ņāü Ļ┤Ćņ░░ļÉśļŖö Ļ▓ā ļō▒ņØ┤ ņ׳ņŚłņ£╝ļ®░,30,33,34 ņ┤Ø ļ│æļ│Ć Ļ░£ņłśņØś 40% ņØ┤ņāü CVS ĻĖ░ņżĆņØä ĒÖ£ņÜ®ĒĢĀ Ļ▓ĮņÜ░ ļ╣äMSņÖĆņØś Ļ░Éļ│äņ¦äļŗ© ļ»╝Ļ░ÉļÅäļŖö 61.3%, ĒŖ╣ņØ┤ļÅäļŖö 84.1%ļĪ£ ĒÖĢņØĖļÉśņŚłļŗż.35
ņāüņ×Éņä▒ ĒģīļæÉļ”¼ ļ│æļ│Ć(paramagnetic rim lesion, PRL)
MS ņØ┤ĒÖś ĻĖ░Ļ░äņØ┤ ņśżļלļÉśĻ▒░ļéś ņ¦äĒ¢ēņä▒ MSņØĖ Ļ▓ĮņÜ░ ļ│æļ│Ć Ļ░Ćņןņ×Éļ”¼ņŚÉņä£ ļ¦īņä▒ ĒÖ£ļÅÖņä▒ Ēāłņłśņ┤łņÖĆ ņČĢņéŁņåīņŗżņØ┤ ņ¦ĆņåŹļÉśļ®░ ĒĢ┤ļŗ╣ ļČĆņ£äņŚÉ ļåÆņØĆ ņ▓ĀņØä ĒĢ©ņ£ĀĒĢśĻ│Ā ņ׳ļŖö(iron-enriched) CD68+ ļ»ĖņäĖņĢäĻĄÉņäĖĒżņÖĆ ļīĆņŗØņäĖĒżņØś ņ╣©ņ£żņØ┤ ļ░£Ļ▓¼ļÉśņŚłļŖöļŹ░ ņØ┤ļ¤¼ĒĢ£ ņĪ░ņ¦üĒĢÖņĀü ĒŖ╣ņ¦ĢņØ┤ ņ×ÉĒÖöņ£©ĻĖ░ļ░śņśüņāüņŚÉņä£ MSĒīÉ ņŻ╝ļ│ĆļČĆļź╝ Ļ░ÉņŗĖĻ│Ā ņ׳ļŖö ĒśĢĒā£ņØś ņĀĆņŗĀĒśĖĻ░ĢļÅä ĒģīļæÉļ”¼ļĪ£ ļ│┤ņØ┤Ļ▓ī ļÉśĻ│Ā ņØ┤ļź╝ iron-rim sign, PRL ļśÉļŖö iron-rim lesion ļō▒ņ£╝ļĪ£ ļČĆļź┤Ļ│Ā ņ׳ļŗż.36-38 ņĄ£ĻĘ╝ ņŚ░ĻĄ¼ņŚÉņä£ļŖö 39-66%ņØś MS ĒÖśņ×ÉņŚÉņä£ ņĄ£ņåī 1Ļ░£ ņØ┤ņāüņØś PRLņØ┤ Ļ┤Ćņ░░ļÉ£ļŗżĻ│Ā ĒĢśļ®░, CVSņÖĆ ļ¦łņ░¼Ļ░Ćņ¦ĆļĪ£ ņ×¼ļ░£ņÖäĒÖöĒśĢ, ņ¦äĒ¢ēĒśĢ MS ļ¬©ļæÉņŚÉņä£ Ļ┤Ćņ░░ļÉśĻ│Ā ļ╣äMSņÖĆ ĻĄ¼ļČäļÉśļŖö ņżæņÜöĒĢ£ ņśüņāüĒĢÖņĀü ĒŖ╣ņ¦Ģņ£╝ļĪ£ ņĀ£ņŗ£ļÉśĻ│Ā ņ׳ļŗż.39
Ļ▓░ļĪĀ
MSņØś ņĀĢĒÖĢĒĢ£ ņ¦äļŗ©ņØä ņ£äĒĢ┤ņä£ļŖö McDonald ņ¦äļŗ© ĻĖ░ņżĆ ņżæ DIS, DIT ņĀĢņØśļź╝ ņל ņØ┤ĒĢ┤ĒĢśĻ│Ā ņĀĢĒÖĢĒĢśĻ▓ī ņĀüņÜ®ĒĢ┤ņĢ╝ ĒĢ£ļŗż. ļśÉĒĢ£ MS ĒŖ╣ņ¦ĢņĀüņØĖ MRI ļ│æļ│Ć ĒśĢĒā£ņÖĆ ņ£äņ╣śļź╝ ņל ņĢīĻ│Ā ņ׳ņ¢┤ņĢ╝ MSņÖĆ ņ£Āņé¼ĒĢ£ ņżæņČöņŗĀĻ▓ĮĻ│ä ņŚ╝ņ”Øņä▒ Ēāłņłśņ┤łņ¦łĒÖśĻ│╝ Ēś╝ļÅÖņØä ļ¦ēĻ│Ā ņśżņ¦äņ£©ņØä ļé«ņČ£ ņłś ņ׳ļŗż. ļ│æļ│Ć Ļ░£ņłśĻ░Ć ņĀüņØä Ļ▓ĮņÜ░ņŚÉļŖö ļ│æļ│Ć Ēü¼ĻĖ░(ņĄ£ņåī 3 mm ņØ┤ņāü), ļ¬©ņ¢æ(ĒāĆņøÉĒśĢ ļśÉļŖö ņøÉĒśĢ), ļ░░ņŚ┤(Ļ░Ćņ¬Į ļćīņŗż ĻĖ░ņżĆ ņłśņ¦üļ░®Ē¢ź)ņØ┤ MSņŚÉ ļČĆĒĢ®ĒĢśļŖöņ¦Ć ņé┤ĒÄ┤ļ│┤Ļ│Ā, ļ│æļ│Ć Ļ░£ņłśĻ░Ć ļ¦ÄņØä Ļ▓ĮņÜ░ņŚÉļŖö ļ│æļ│Ć ņ£äņ╣śņÖĆ ļČäĒżĻ░Ć MSņŚÉ ļČĆĒĢ®ĒĢśļŖöņ¦Ć ņé┤ĒÄ┤ļ│┤ļŖö Ļ▓ī ļÅäņøĆņØ┤ ļÉĀ ņłś ņ׳ļŗż.10 ļ¦łņ¦Ćļ¦ēņ£╝ļĪ£ CVSņÖĆ PRLņØĆ ņāłļĪŁĻ▓ī ļČĆņāüĒĢśĻ│Ā ņ׳ļŖö MSņØś MRI ĒŖ╣ņ¦ĢņØ┤ļ»ĆļĪ£ ņØ┤ņŚÉ ļīĆĒĢ┤ ņל ņØ┤ĒĢ┤ĒĢ┤ļæÉĻ│Ā Ē¢źĒøä ņ¦äļŗ© ĻĖ░ņżĆņŚÉ ĒżĒĢ©ļÉśļŖöņ¦Ć ņ¦Ćņ╝£ļ│╝ ĒĢäņÜöĻ░Ć ņ׳Ļ▓Āļŗż.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



