

ņä£ļĪĀ
ņżæņČöņŗĀĻ▓ĮĻ│ä ņŚ╝ņ”Øņä▒ ņ¦łĒÖśņŚÉļŖö ļīĆĒæ£ņĀüņ£╝ļĪ£ ļŗżļ░£Ļ▓ĮĒÖöņ”Ø, ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝, ĒĢŁņłśņ┤łĒؼņåīļÅīĻĖ░ņĢäĻĄÉņäĖĒżļŗ╣ļŗ©ļ░▒ņ¦łĒĢŁņ▓┤ Ļ┤ĆļĀ© ņ¦łĒÖś(myelin oligodendrocyte glycoprotein antibody-associated disease, MOGAD)Ļ│╝ ņåīņĢäņŚÉņä£ ĒØöĒĢ£ ĻĖēņä▒Ēīīņóģņä▒ļćīņ▓ÖņłśņŚ╝(acute disseminated encephalomyelitis, ADEM)ņØ┤ ņ׳ņ£╝ļ®░, ĻĘĖ ņÖĖņŚÉļÅä ņĀäņŗĀĒÖŹļ░śļŻ©ĒæĖņŖżņØ┤ļéś ņć╝ĻĘĖļĀīņ”ØĒøäĻĄ░, ļ▓Āņ▓┤ĒŖĖļ│æ, ņé¼ļź┤ņĮöņØ┤ļō£ņ”Ø ļō▒ļÅä ņżæņČöņŗĀĻ▓ĮĻ│äļź╝ ņ╣©ļ▓öĒĢĀ ņłś ņ׳ļŗż.1 ĻĘĖ ņÖĖņŚÉļÅä ņ×ÉĻ░Ćļ®┤ņŚŁ ļćīņŚ╝ņØ┤ļéś ņØ╝ļČĆ Ļ░ÉņŚ╝ņä▒ ņ¦łĒÖśņØ┤ļéś ļīĆņé¼ņä▒ ņ¦łĒÖśņŚÉ ņØśĒĢ┤ņä£ļÅä ņżæņČöņŗĀĻ▓ĮĻ│ä ņŚ╝ņ”Øņä▒ ņ¦łĒÖśņØä ņ£Āļ░£ļÉĀ ņłś ņ׳ņ£╝ļ®░, ņĄ£ĻĘ╝ņŚÉļŖö ļ®┤ņŚŁĻ┤Ćļ¼Ė ņ¢ĄņĀ£ņĀ£(immune checkpoint inhibitors)ņŚÉ ņØśĒĢ£ ļ│┤Ļ│ĀļÅä ņ׳ļŗż.2 ņ×äņāü ņ¢æņāüĻ│╝ ļ│æļĀź, ņŗĀĻ▓ĮĒĢÖņĀü ņ¦äņ░░ņØĆ ņ¦äļŗ©ņŚÉ ļ¦żņÜ░ ņżæņÜöĒĢśļéś ļĢīļĪ£ļŖö ņĀ£ĒĢ£ņĀüņØ╝ ņłś ņ׳ņ¢┤ņä£, Ļ░ü ņ¦łĒÖśļ│ä ņśüņāüĒĢÖņĀü ĒŖ╣ņ¦ĢĻ│╝ ņ░©ņØ┤ļź╝ ņĢäļŖö Ļ▓āņØ┤ ņżæņČöņŗĀĻ▓ĮĻ│ä ņŚ╝ņ”Øņä▒ ņ¦łĒÖśļōżņØś Ļ░Éļ│ä ņ¦äļŗ©ņŚÉ ĒĢäņÜöĒĢśĻ▓Āļŗż. ņØ┤ ļģ╝ļ¼ĖņŚÉņä£ļŖö ļŗżļ░£Ļ▓ĮĒÖöņ”Ø, ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņÖĆ MOGADņŚÉņä£ ļ░£ņāØĒĢśļŖö ņŗ£ņŗĀĻ▓ĮņŚ╝, ļćīļ│æļ│Ć ļ░Å ņ▓ÖņłśņŚ╝ņØś ņ×ÉĻĖ░Ļ│Ąļ¬ģņśüņāü(MRI)ņØś ĒŖ╣ņ¦ĢņØä ņżæņĀÉņ£╝ļĪ£ ņé┤ĒÄ┤ļ│┤Ļ│Ā, ļŗżņ¢æĒĢ£ ņżæņČöņŗĀĻ▓ĮĻ│ä ņŚ╝ņ”Øņä▒ ņ¦łĒÖśņØś ĒŖ╣ņ¦ĢņĀüņØĖ ņåīĻ▓¼ļōżņØä Ļ░äļץĒ׳ ņåīĻ░£ĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ļ│ĖļĪĀ
ļŗżļ░£Ļ▓ĮĒÖöņ”Ø, ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝Ļ│╝ MOGADņŚÉņä£ ņŗ£ņŗĀĻ▓ĮņŚ╝ņØś ņśüņāüĒĢÖņĀü ĒŖ╣ņ¦Ģ
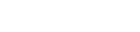
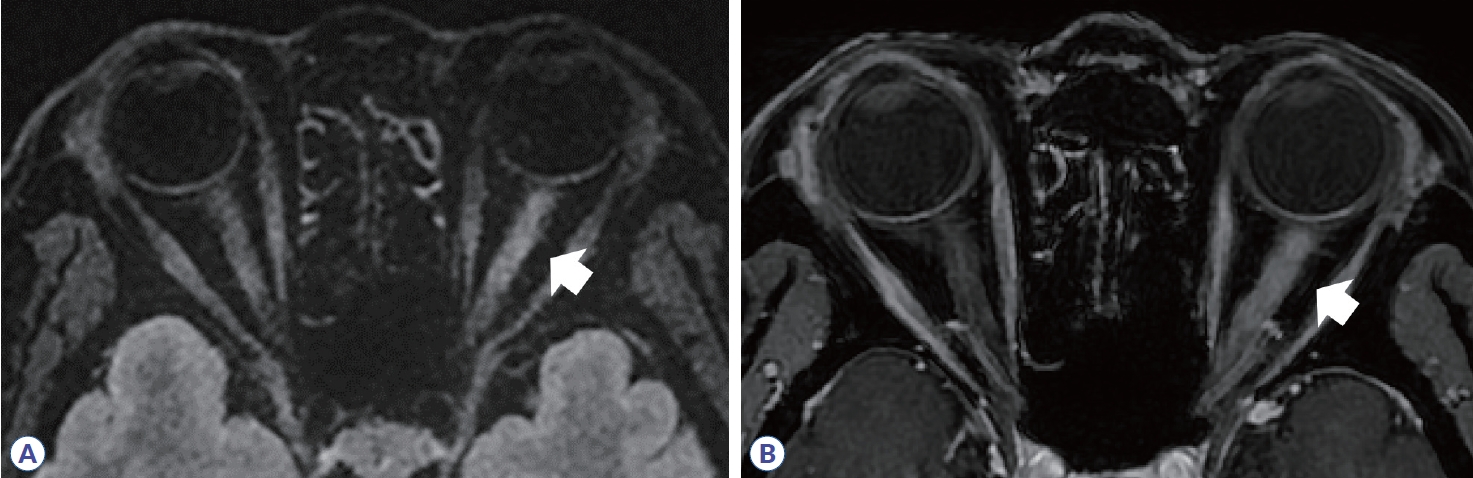
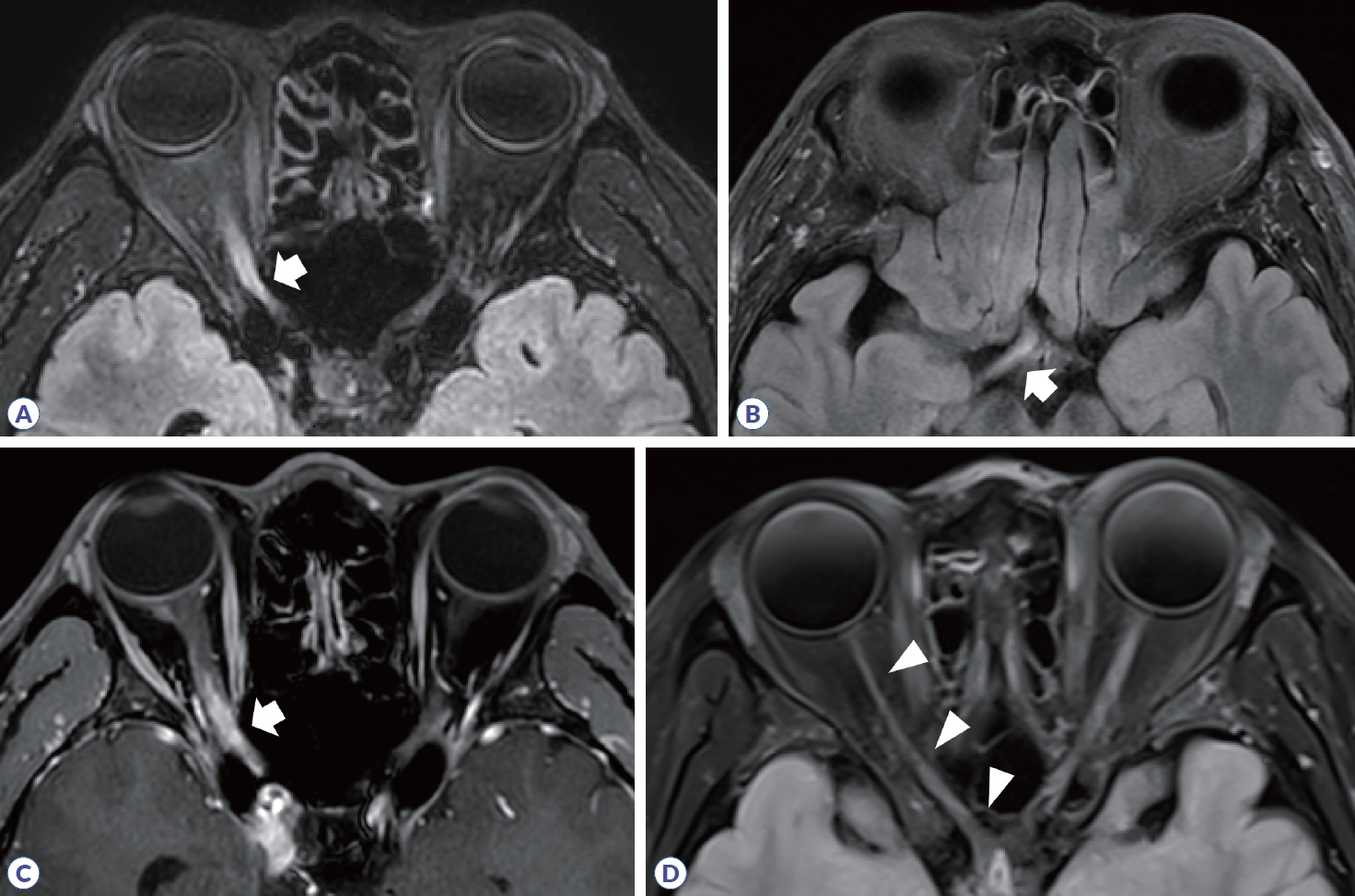
ņŗ£ņŗĀĻ▓ĮņŚ╝ņØĆ ļŗżļ░£Ļ▓ĮĒÖöņ”ØņŚÉņä£ ņ┤łĻĖ░ ņ”Øņāüņ£╝ļĪ£ 25%, ņĀäņ▓┤ ņ¦łļ│æ Ļ▓ĮĻ│╝ņØś 70%Ļ╣īņ¦Ć ņ░©ņ¦ĆĒĢśĻ│Ā ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝Ļ│╝ MOGADņŚÉņä£ļÅä ĒØöĒĢśĻ▓ī ļ░£ņāØĒĢśļ®░, ņŗ£ļĀź ņĀĆĒĢśņÖĆ ņāēĻ░ü Ļ░Éņåī, ņŗ£ņĢ╝ņןņĢĀņØś ņ”ØņāüņØä ļÅÖļ░śĒĢ£ļŗż.3 ļŗżļ░£Ļ▓ĮĒÖöņ”ØņŚÉņä£ ļ░£ņāØĒĢśļŖö ņŗ£ņŗĀĻ▓ĮņŚ╝ņØś ņĀäĒśĢņĀüņØĖ ņśüņāüĒĢÖņĀü ņåīĻ▓¼ņØĆ ļ│æļ│ĆņØ┤ ņŻ╝ļĪ£ ĒÄĖņĖĪņ£╝ļĪ£ ļ░£ņāØĒĢśĻ│Ā, ļīĆļČĆļČä canalicular segmentņŚÉ ņ£äņ╣śĒĢśļ®░, ļ│æļ│ĆņØś ĻĖĖņØ┤Ļ░Ć ņĀäņ▓┤ ņŗ£ņŗĀĻ▓ĮņØś 1/2 ļ»Ėļ¦īņ£╝ļĪ£ ņ¦¦ļŗż(Fig. 1, Table 1). ņŖżņø©ļŹ┤ ņŚ░ĻĄ¼ņŚÉņä£ 472ļ¬ģņØś ļŗżļ░£Ļ▓ĮĒÖöņ”Ø ĒÖśņ×ÉļōżņØä ļ│┤Ļ│ĀĒĢ£ ļ░öņŚÉ ļö░ļź┤ļ®┤ ņĢĮ 21%ņŚÉņä£ ņ▓½ ņ”Øņāüņ£╝ļĪ£ ņŗ£ņŗĀĻ▓ĮņŚ╝ņØ┤ ļ░£ņāØĒĢśņśĆĻ│Ā, ņĀäņ▓┤ Ļ▓ĮĻ│╝ ņżæņŚÉ ņ¢æņĢł ļ¬©ļæÉ ņŗ£ņŗĀĻ▓ĮņŚ╝ņØ┤ ļ░£ņāØĒĢ£ Ļ▓ĮņÜ░ļŖö ņĢĮ 5.5%ņśĆņ£╝ļéś ļÅÖņŗ£ņŚÉ ņ¢æņĖĪ ņŗ£ņŗĀĻ▓ĮņŚ╝ņØ┤ ļ░£ņāØĒĢśļŖö Ļ▓ĮņÜ░ļŖö 0.42%ļĪ£ ļ¦żņÜ░ ļō£ļ¼╝Ļ▓ī ļ│┤Ļ│ĀļÉśņŚłļŗż. ņØ┤ņŚÉ ļ░śĒĢ┤ ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝Ļ│╝ MOGADņŚÉņä£ļŖö ņĢĮ 30-35%ņŚÉņä£ ļÅÖņŗ£ņŚÉ ņ¢æņĖĪ ņŗ£ņŗĀĻ▓ĮņŚ╝ņØ┤ ļ░£ņāØĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ņ£╝ļ®░, ļ│æļ│ĆņØś ĻĖĖņØ┤ļÅä ņĀäņ▓┤ ņŗ£ņŗĀĻ▓ĮņØś 1/2ļ│┤ļŗż ĻĖ┤ ļ│æļ│ĆņØä Ļ░Ćņ¦ĆļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äļŗż(Figs. 2, 3). ņĢłĻĄ¼ MRIņŚÉņä£ ņŗ£ņŗĀĻ▓Į ņ▓ÖņłśņŚ╝ņØ┤ļéś MOGADņØś ņŗ£ņŗĀĻ▓ĮņŚ╝ ļ│æļ│Ć ĻĖĖņØ┤ļŖö ļŗżļ░£Ļ▓ĮĒÖöņ”ØņŚÉ ļ╣äĒĢ┤ ņĢĮ 2-3ļ░░ņØś ĻĖĖņŚłļŗż.4,5 ņŗ£ņŗĀĻ▓ĮņŚ╝ņØś ĒśĖļ░£ ļČĆņ£äļÅä ņ¦łļ│æ Ļ░ä ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ļŖöļŹ░, ņŗ£ņŗĀĻ▓ĮĻĄÉņ░©(optic chiasm)ļź╝ ņ╣©ļ▓öĒĢśļŖö Ļ▓ĮņÜ░Ļ░Ć ļŗżļ░£Ļ▓ĮĒÖöņ”ØņØ┤ļéś MOGADņŚÉņä£ļŖö 2-15%ņśĆņ£╝ļéś ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņØś Ļ▓ĮņÜ░ ņĢĮ 64%ļĪ£ ļ¦żņÜ░ ļåÆĻ▓ī ļéśĒāĆļé¼ļŗż. MOGADņŚÉņä£ļŖö ņāüļīĆņĀüņ£╝ļĪ£ ņŗ£ņŗĀĻ▓Į ņĢ×ņ¬ĮļČäņĀłņØä ņ╣©ļ▓öĒĢśļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦ÄņĢśņ£╝ļ®░, ņŗ£ņŗĀĻ▓Į ņ£ĀļæÉ ļČĆņóģļÅä ļ¦ÄĻ▓īļŖö ņĢĮ 50%ņŚÉņä£ ļ│┤Ļ│ĀļÉśņŚłļŗż. ļśÉĒĢ£ ņĪ░ņśüņ”ØĻ░Ģ ņśüņāüņŚÉņä£ ņŗĀĻ▓ĮņŻ╝ņ£ä ņĪ░ņśüņ”ØĻ░Ģ(perineural enhancement)ņØ┤ Ļ┤Ćņ░░ļÉĀ ņłś ņ׳ļŗż(Fig. 3, Table 1).
ņ×ÉĻĖ░Ļ│Ąļ¬ģņśüņāüņØś ĒŖ╣ņłśĻĖ░ļ▓Ģņ£╝ļĪ£ ņ¢╗ņØĆ ņ×ÉĻĖ░ĒÖöņĀäļŗ¼ļ╣äņ£©(magnetization transfer ratio, MTR)ļÅä ņ¦łĒÖśļōżņØś Ļ░Éļ│äņŚÉ ļÅäņøĆņØ┤ ļÉśļŖö ļŹ░, ņØ┤ļŖö ņ×ÉĻĖ░ĒÖöņĀäļŗ¼ĒīīņŚÉ ļīĆĒĢ┤, ņ×Éņ£ĀļĪ£ņØ┤ ņøĆņ¦üņØ┤ļŖö ļ¼╝ļČäņ×ÉņÖĆ ņłśņ┤ł(myelin) Ēś╣ņØĆ ņČĢņéŁļ¦ē(axon membrane)ņŚÉ ļČÖņ¢┤ ņ׳ļŖö ņāüĒā£ņØś ļ¼╝ļČäņ×ÉĻ░Ć ļŗżļźĖ ĒŖ╣ņä▒ņØä ļ│┤ņØ┤ļŖö Ļ▓āņØä ņØ┤ņÜ®ĒĢśņŚ¼ Ļ│äņé░ĒĢ£ Ļ▓āņØ┤ļŗż. ļćīņ▓ÖņłśņĢĪņŚÉņä£ļŖö MTRņØ┤ 0ņŚÉ ņłśļĀ┤ĒĢśļ®░, ņĀĢņāü ļćīņĪ░ņ¦üņŚÉņä£ļŖö ņĢĮ 40-50ņØä ļ│┤ņØ┤ļŖöļŹ░, ņŗĀĻ▓Į ņåÉņāüņØ┤ ļ░£ņāØĒĢśļ®┤ MTRņØ┤ Ļ░ÉņåīĒĢ£ļŗż.6 ļŗżļ░£Ļ▓ĮĒÖöņ”ØņŚÉņä£ ņŗ£ņŗĀĻ▓ĮņŚ╝ņØ┤ ļ░£ņāØĒĢ£ Ļ▓ĮņÜ░ ļ│æļ│Ć ļČĆņ£äņØś MTRņØ┤ ņ”Øņāü ļ░£ņāØ 8Ļ░£ņøö ļÆż Ļ░Ćņן ļé«Ļ│Ā(nadir) ņØ┤Ēøä ņä£ņä£Ē׳ ĒśĖņĀäļÉśļŖö ņČöņØ┤ļź╝ ļ│┤ņØĖļŗż.7 ļŗżļ░£Ļ▓ĮĒÖöņ”ØņŚÉ ļ╣äĒĢ┤ ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņØ┤ļéś MOGADņŚÉņä£ļŖö MTRņØś Ļ░ÉņåīĻ░Ć ļŹö ņŗ¼ĒĢ£ Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż.8
ņĢłĻĄ¼ļ╣øĻ░äņäŁļŗ©ņĖĄņ┤¼ņśü(optical coherence tomography, OCT)ņØĆ ļ¦Øļ¦ē ņŗ£ņŗĀĻ▓ĮņĖĄņØś ļæÉĻ╗śļź╝ ĒÅēĻ░ĆĒĢśļŖö ļŹ░ ņØ┤ņÜ®ĒĢĀ ņłś ņ׳ņ£╝ļ®░, ņŗĀĻ▓ĮņĀłņäĖĒż(ganglion cell)ņØś ņČĢņéŁņØ┤ ļ¬©ņØ┤ļŖö ņŗ£ņŗĀĻ▓Įņ£ĀļæÉņØś ļ¦Øļ¦ēņŗĀĻ▓Įņä¼ņ£ĀņĖĄ(retinal nerve fiber layer, RNFL)Ļ│╝ ĒÖ®ļ░ś ņŗĀĻ▓ĮņĀłņäĖĒż-ļé┤ļ¦ØņāüņĖĄ(ganglion cell-inner plexiform layer, GCIP)ņØś ļæÉĻ╗śļź╝ ņŻ╝ļĪ£ ņĖĪņĀĢĒĢ£ļŗż.9 ņŗ£ņŗĀĻ▓ĮņŚ╝ ĻĖēņä▒ĻĖ░ņŚÉļŖö ļ¦Øļ¦ē ļČĆņóģņ£╝ļĪ£ ņØĖĒĢ┤ OCTņŚÉņä£ ņŗ£ņŗĀĻ▓ĮņĖĄņØ┤ ļæÉĻ║╝ņøīņ¦ä Ļ▓āņØ┤ Ļ┤Ćņ░░ļÉ£ļŗż. ņŗ£ņŗĀĻ▓ĮņŚ╝ņØ┤ ļ░£ņāØĒĢ£ MOGADņØś 31Ļ░£ņÖĆ ļŗżļ░£Ļ▓ĮĒÖöņ”ØņØś 48Ļ░£ ļłłļōżņØä ņĀĢņāüņĖĪ ļłłņŚÉ ļ╣äĻĄÉĒĢśņśĆņØä ļĢī, GCIP ļæÉĻ╗śļŖö ņ░©ņØ┤Ļ░Ć ņŚåņŚłņ£╝ļéś RNFLņØś ļæÉĻ╗śļŖö ņ£ĀņØśĒĢśĻ▓ī ļæÉĻ║╝ņøīņĀĖ ņ׳ņ£╝ļ®░, ĒŖ╣Ē׳ MOGADņŚÉņä£ļŖö RNFLņØś ņżæņĢÖĻ░ÆņØ┤ 45 ╬╝m (interquartile rage [IQR], 17-105)ļĪ£ ļŗżļ░£Ļ▓ĮĒÖöņ”Ø(ņżæņĢÖĻ░Æ, 7.5; IQR, 1-18)ņŚÉ ļ╣äĒĢ┤ ņĢĮ 6ļ░░ ļåÆņĢśļŗż.10 ļ╣øĻ░äņäŁļŗ©ņĖĄĒśłĻ┤ĆņĪ░ņśüņłĀ(OCT angiography)ņŚÉņä£ļŖö ļŗżļ░£Ļ▓ĮĒÖöņ”ØņØ┤ļéś ņŗ£ņŗĀĻ▓Į ņ▓ÖņłśņŚ╝ņŚÉņä£ ļ│æļ│ĆņĖĪ ļłłņØ┤ ņĀĢņāüņĖĪ ļłłņŚÉ ļ╣äĒĢ┤ ņ£ĀļæÉņŻ╝ļ│Ćļ¬©ņäĖĒśłĻ┤Ćņ┤Ø(peripapillary capillary plexus)ņØś ļ░ĆļÅäĻ░Ć Ļ░ÉņåīĒĢśņśĆņ£╝ļ®░, ņØ┤ļŖö ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņŚÉņä£ ļŹöņÜ▒ ļÜ£ļĀĘĒĢśņśĆļŗż.11
ļŗżļ░£Ļ▓ĮĒÖöņ”Ø, ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝Ļ│╝ MOGADņŚÉņä£ ļćīļ│æļ│ĆņØś ņśüņāüĒĢÖņĀü ĒŖ╣ņ¦Ģ
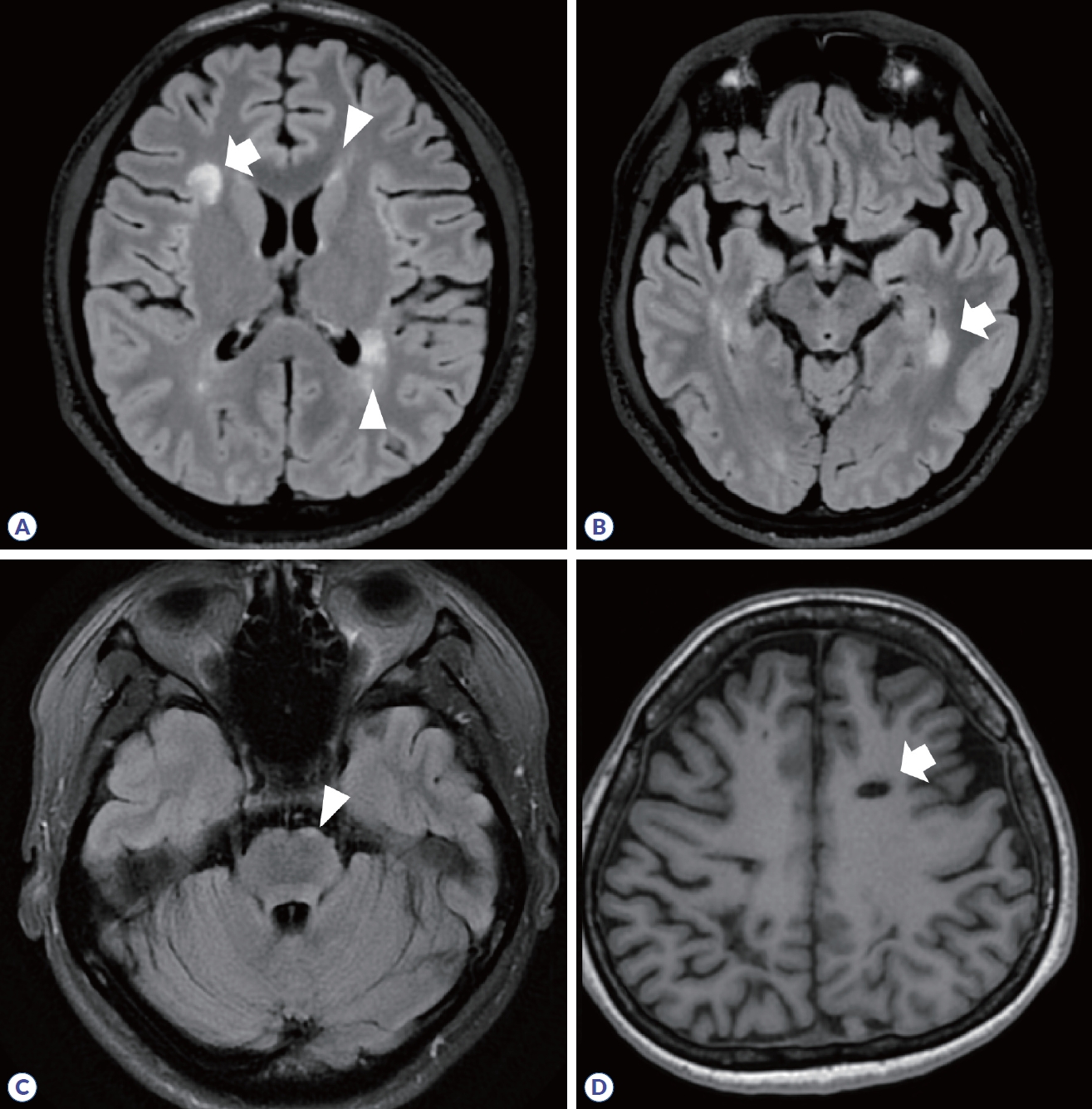
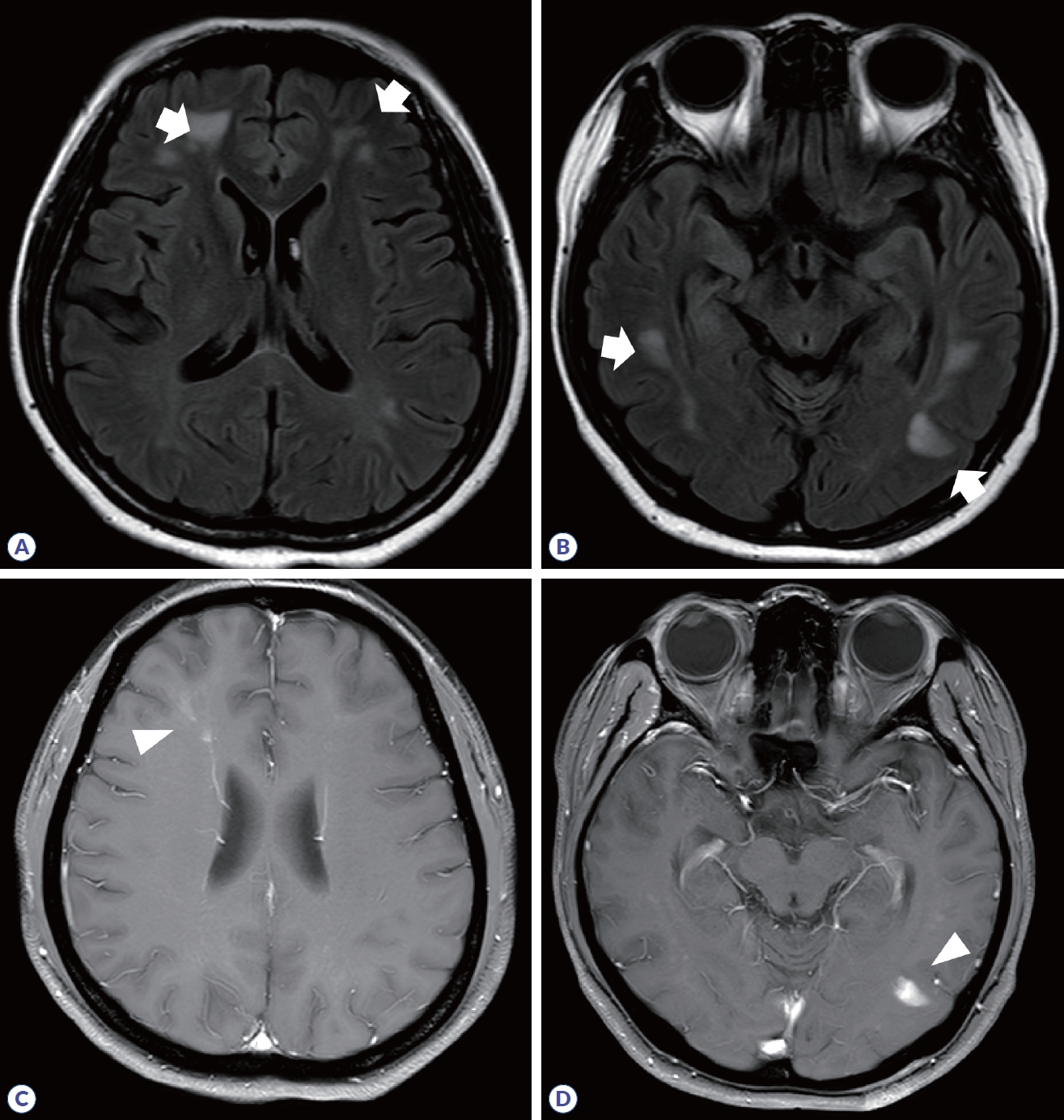
ļŗżļ░£Ļ▓ĮĒÖöņ”ØņØĆ 2017 McDonald ņ¦äļŗ© ĻĖ░ņżĆņŚÉņä£ ļćīļ│æļ│ĆņØĆ ņ¦äļŗ©ņŚÉ ĒĢäņłśņĀüņØ┤ļ®░, Ēö╝ņ¦ł/Ēö╝ņ¦łĻ│ü(cortical/juxtacortical), ļćīņŗżņŻ╝ņ£ä(periventricular), ņ▓£ļ¦ēļ░æ(infratentorial)ņŚÉ Ēāłņłśņ┤ł ļ│æļ│ĆņØ┤ ĒÖĢņØĖļÉśļŖö Ļ▓ĮņÜ░ļĪ£ ņĀ£ņŗ£ļÉśņŚłļŗż(Fig. 4, Table 2).12 ņĀäĒśĢņĀüņØĖ ļ│æļ│ĆņØś Ļ▓ĮņÜ░, Ļ▓ĮĻ│äĻ░Ć ļ¬ģĒÖĢĒĢ£ ĒāĆņøÉ Ēś╣ņØĆ ņøÉĒśĢ ļ¬©ņ¢æņØ┤ļ®░, ņĪ░ņśüņ”ØĻ░Ģ ņśüņāüņŚÉņä£ ĻĘĀņ¦łĒĢśĻ▓ī ņĪ░ņśüņ”ØĻ░ĢļÉśĻ▒░ļéś Ļ│Āļ”¼(ring) Ēś╣ņØĆ ņŚ┤ļ”░Ļ│Āļ”¼(open-ring)ļĪ£ ļéśĒāĆļé£ļŗż.13,14 Ļ░Ćņ¬Įļćīņŗż ņŻ╝ņ£äņŚÉ ļ│æļ│ĆņØ┤ ļ░£ņāØĒĢśļ®┤ ņåÉĻ░ĆļØĮņØś ļ¬©ņ¢æĻ│╝ ņ£Āņé¼ĒĢśņŚ¼ DawsonŌĆÖs fingerļØ╝Ļ│ĀļÅä ĒĢ£ļŗż. ļ│æļ│ĆņØ┤ ļ░£ņāØĒ¢łļŹś ļČĆņ£äņŚÉļŖö ņŗ£Ļ░äņØ┤ ņ¦Ćļéśļ®┤ ņĪ░ņ¦ü ņåīņŗż(tissue loss)ļĪ£ ņØĖĒĢ┤ T1 Ļ░ĢņĪ░ņśüņāüņŚÉņä£ Ļ▓ĆĻ▓ī ļ│┤ņØ┤ļŖö Ļ▓ĆņØĆĻĄ¼ļ®Ź(T1-black hole)ņØ┤ Ļ┤Ćņ░░ļÉĀ ņłś ņ׳ļŗż(Fig. 4D). ļśÉĒĢ£, ņĢäļלņĖĪļæÉņŚĮ ļćīņŗż ņŻ╝ļ│ĆņŚÉ ļ│æļ│ĆņØ┤ ņāØĻĖ░ļŖö Ļ▓ĮņÜ░ ļŗżļ░£Ļ▓ĮĒÖöņ”ØņØś Ļ░ĆļŖźņä▒ņØä ņóĆ ļŹö ņŗ£ņé¼ĒĢ£ļŗż(Fig. 4B).
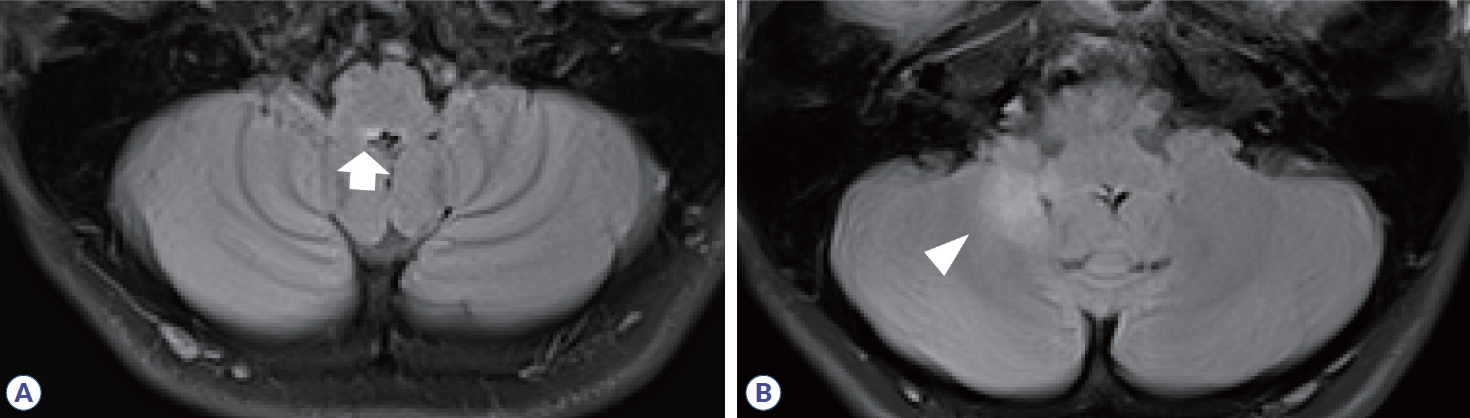
ļŗżļ░£Ļ▓ĮĒÖöņ”ØĻ│╝ ļŗ¼ļ”¼ ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņØ┤ļéś MOGADņŚÉņä£ļŖö ņ¦äļŗ©ņŚÉ ļćīļ│æļ│ĆņØ┤ ĒĢäņłśņĀüņØ┤ņ¦ĆļŖö ņĢŖņ£╝ļ®░, ļćīļ│æļ│ĆņØś ņ£Āļ¼┤ļŖö ņ¦äļŗ© ņŗ£ Ļ░üĻ░ü 23-30%ņÖĆ 27-44%ļĪ£ ļ│┤Ļ│ĀļÉśņŚłļŗż.8,15 ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņŚÉņä£ ļćīļ│æļ│ĆņØĆ ņŻ╝ļĪ£ ļćīņŗż ņŻ╝ļ│ĆņØä ļö░ļØ╝ ļ░£ņāØĒĢśļŖöļŹ░, ņĀ£3ļćīņŗżĻ│╝ ļīĆļćīņłśļÅä, ņŗ£ņāü, ņŗ£ņāüĒĢśļČĆ, ņĀ£4ļćīņŗż ņŻ╝ļ│ĆņØś ļćīĻ░äņŚÉ ĒśĖļ░£ĒĢśļ®░, ļ¦©ņĢäļלĻĄ¼ņŚŁ(area postrema)ņØä ĒżĒĢ©ĒĢ£ ļō▒ņ¬Įņł©ļćī(dorsal medulla)ņŚÉ ņāØĻĖ┤ ļ│æļ│ĆņØĆ Ļ▓ĮņłśĻ╣īņ¦Ć ņØ┤ņ¢┤ņ¦ĆĻĖ░ļÅä ĒĢ£ļŗż(Fig. 5).16 Ļ░ĆņĖĪļćīņŗż ņŻ╝ļ│Ć ļćīļ¤ē ļ│æļ│Ć(callosal lesion)ņØĆ ļćīņŗżļ¦ēļé┤ņĖĄ(ependymal lining)ņØä ļö░ļØ╝ ļ░£ņāØĒĢśņŚ¼ ŌĆśmarbleŌĆÖ Ēś╣ņØĆ ŌĆśarch bridge patternŌĆÖņØ┤ļØ╝ ĒĢ£ļŗż. ļ│æļ│ĆņØś ļ¬©ņ¢æņØĆ ļŗżļ░£Ļ▓ĮĒÖöņ”ØĻ│╝ ļŗ¼ļ”¼ ņל ņĀĢĒśĢĒÖöļÉśņ¦Ć ņĢŖņ£╝ļ®░, ĒśłĻ┤Ćņä▒ ļČĆņóģ(vasogenic edema)ņØä ļÅÖļ░śĒĢśĻ▒░ļéś ņóģĻ┤┤ņ¢æ(tumefactive) ļ¬©ņŖĄņ£╝ļĪ£ ļ│┤ņØ╝ ņłś ņ׳Ļ│Ā, ļ¦īņä▒ĒÖöļÉ£ Ļ▓ĮņÜ░ ļéŁņóģņ£Āņé¼ Ļ│ĄļÅÖ ļ│ĆĒÖö(cystic-like cavity change)Ļ░Ć ļÅÖļ░śļÉĀ ņłś ņ׳ļŗż. ļśÉĒĢ£, ĒÄĖņĖĪ Ēś╣ņØĆ ņ¢æņĖĪ Ēö╝ņ¦łņ▓ÖņłśļĪ£ļź╝ ļö░ļØ╝ ļ│æļ│ĆņØ┤ ņāØĻĖ░ļŖö Ļ▓ĮņÜ░ ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņØś Ļ░ĆļŖźņä▒ņØä ņŗ£ņé¼ĒĢ£ļŗż. ņĪ░ņśüņ”ØĻ░ĢņØĆ cloud-like Ēś╣ņØĆ linearĒĢ£ ņ¢æņāüņØ┤ļ®░, ļćīņłśļ¦ē ņĪ░ņśüņ”ØĻ░ĢļÅä ļÅÖļ░śļÉĀ ņłś ņ׳ļŗż(Table 2). MOGADņŚÉņä£ ļćīļ│æļ│ĆņØĆ ADEMĻ│╝ ņ£Āņé¼ĒĢśĻ▓ī ļéśĒāĆļéśļ®░, ļ░▒ņ¦ł, Ļ╣ŖņØĆĒÜīņāēņ¦ł, ņåīļćīņżæĻ░äļŗżļ”¼, ļćīĻ░ä, Ēö╝ņ¦łņŚÉ ļ│æļ│ĆņØś Ļ▓ĮĻ│äĻ░Ć ļČłļ¬ģĒÖĢĒĢśĻ│Ā ņ£ĄĒĢ®ņä▒(confluent) ļ│æļ│ĆņØ┤ Ļ┤Ćņ░░ļÉ£ļŗż(Fig. 6).17 ņĪ░ņśüņ”ØĻ░ĢņØĆ ļÅÖļ░śļÉśņ¦Ć ņĢŖĻĖ░ļÅä ĒĢśĻ│Ā, ĒÄĖņĖĪ Ēś╣ņØĆ ņ¢æņĖĪ Ēö╝ņ¦ł ņŚ░ņłśļ¦ē ņĪ░ņśüņ”ØĻ░ĢņØä ļéśĒāĆļéśĻĖ░ļÅä ĒĢ£ļŗż.
ņØ┤ļ¤¼ĒĢ£ ļ│æļ│ĆņØś ņ£äņ╣śļéś ļ¬©ņ¢æņØĆ ņ¦łļ│æļōżņØä ņä£ļĪ£ ĻĄ¼ļČäĒĢśļŖö ļŹ░ ļ¦żņÜ░ ņżæņÜöĒĢ£ ĻĖ░ņżĆņØ┤ ļÉ£ļŗż(Table 2). ņĢäļלņĖĪļæÉņŚĮ ļćīņŗż ņŻ╝ņ£ä ļ│æļ│ĆĻ│╝ Uņä¼ņ£Ā ļ│æļ│Ć, DawsonŌĆÖs finger ļ¬©ļæÉ ļÅÖļ░śĒĢśļŖö Ļ▓ĮņÜ░ņŚÉļŖö ņŗ£ņŗĀĻ▓Į ņ▓ÖņłśņŚ╝Ļ│╝ MOGADņŚÉ ļ╣äĒĢ┤ ļŗżļ░£Ļ▓ĮĒÖöņ”ØņŚÉ ļīĆĒĢ£ ņ¢æņä▒ņśłņĖĪļźĀņØ┤ Ļ░üĻ░ü 90.3%ņÖĆ 97.6%ļĪ£ ļ¦żņÜ░ ļåÆĻ▓ī ļéśĒāĆļé¼ļŗż.18 Ēö╝ņ¦ł ļ│æļ│ĆņØś ņ£Āļ¼┤ļÅä ļŗżļ░£Ļ▓ĮĒÖöņ”ØĻ│╝ ļŗżļźĖ ņżæņČöņŗĀĻ▓ĮĻ│ä ņŚ╝ņ”Øņä▒ ņ¦łĒÖśļōżņØä ĻĄ¼ļČäĒĢśļŖö ļŹ░ ļÅäņøĆņØ┤ ļÉ£ļŗż. Ēö╝ņ¦ł ļ│æļ│ĆņØĆ ĒśĢĒā£ņŚÉ ļö░ļØ╝ 4Ļ░Ćņ¦ĆļĪ£ ĻĄ¼ļČäļÉśļŖöļŹ░ (1ĒśĢ: mixed white and gray matter lesion, 2ĒśĢ: intracortical lesion, 3ĒśĢ: subpial lesion, 4ĒśĢ: ŌĆśworm-like lesion),19 ĒĢśļéś ņØ┤ņāüņØś Ēö╝ņ¦ł ļ│æļ│Ćļ¦ī ņ׳ļŹöļØ╝ļÅä ļŗżļ░£Ļ▓ĮĒÖöņ”ØĻ│╝ ļŗ©ļÅģņ×äņāüņ”ØĒøäĻĄ░ņŚÉ ļīĆĒĢ┤ ļ»╝Ļ░ÉļÅä 59.0%, ĒŖ╣ņØ┤ļÅä 93.6%ņÖĆ ņĀĢĒÖĢņä▒ 73.9%ļź╝ ļ│┤ņśĆļŗż.20 ļŗżļ░£Ļ▓ĮĒÖöņ”ØņØä ņŗ£ņé¼ĒĢśļŖö ļśÉ ļŗżļźĖ ņśüņāü ņåīĻ▓¼ņØĖ ņżæņŗ¼ņĀĢļ¦źņŗĀĒśĖ(central vein sign, CVS)ļŖö 3 mm ņØ┤ņāü Ēü¼ĻĖ░ņØś Ēāłņłśņ┤ł ļ│æļ│Ć ņżæņŗ¼ļČĆļź╝ Ļ┤ĆĒåĄĒĢśļŖö ņ¦üĻ▓Į 2 mm ļ»Ėļ¦īņØś ĒśłĻ┤ĆņØä ņØśļ»ĖĒĢ£ļŗż. CVSĻ░Ć ļćīļ│æļ│ĆņØś 40%ņŚÉ ņĪ┤ņ×¼ĒĢśļŖö Ļ▓āņØä ĻĖ░ņżĆ(cut-off)ņ£╝ļĪ£ ĒĢśņśĆņØä Ļ▓ĮņÜ░, ļŗżļ░£Ļ▓ĮĒÖöņ”Ø ņ¦äļŗ©ņŚÉ ļ»╝Ļ░ÉļÅä 78.7%, ĒŖ╣ņØ┤ļÅä 86.0%, ņĀĢĒÖĢņä▒ 81.5%ļź╝ ļ│┤ņśĆļŗż. ļśÉĒĢ£, ņāüņ×Éņä▒ ĒģīļæÉļ”¼ ļ│æļ│Ć(paramagnetic rim lesion)ņØĆ ļŗżļ░£Ļ▓ĮĒÖöņ”ØņŚÉņä£ ļ│æļ│Ć ņŻ╝ļ│Ć ļ¦īņä▒ņŚ╝ņ”Ø(perilesional chronic inflammation)ņØä ļ░śņśüĒĢśļŖö Ļ▓āņ£╝ļĪ£, ļ│æļ”¼ņĀüņ£╝ļĪ£ļŖö ļ│æļ│Ć Ļ░Ćņןņ×Éļ”¼ņŚÉ ņ▓ĀĒĢ©ņ£Ā ļ»ĖņäĖņĢäĻĄÉņäĖĒż/ļīĆņŗØņäĖĒż(iron-laden microglial/macrophage)Ļ░Ć Ļ┤Ćņ░░ļÉśļ®░, T2* Ļ░ĢņĪ░ņśüņāüņŚÉņä£ ĒĢ┤ļŗ╣ ļČĆļČäņØ┤ ņĀĆĻ░ĢļÅä ņŗĀĒśĖļĪ£ ļéśĒāĆļé£ļŗż.21 ļŗżļźĖ ņżæņČöņŗĀĻ▓ĮĻ│ä ņŚ╝ņ”Øņä▒ ņ¦łĒÖśņØ┤ļéś ļ╣äņŚ╝ņ”Øņä▒ ņ¦łĒÖśņŚÉņä£ļŖö paramagnetic rim lesionņØ┤ ĒĢśļéś ņØ┤ņāü ņĪ┤ņ×¼ĒĢśļŖö Ļ▓ĮņÜ░ļŖö 10% ļ»Ėļ¦īņØ┤ļéś ļŗżļ░£Ļ▓ĮĒÖöņ”ØņŚÉņä£ļŖö ņĢĮ 52-58%ļĪ£ ĒØöĒĢśĻ▓ī ļéśĒāĆļé¼Ļ│Ā, CVS (cut-off value 40%)ņÖĆ Ļ░ÖņØ┤ ņØ┤ņÜ® ņŗ£, ļŗżļ░£Ļ▓ĮĒÖöņ”ØņŚÉ ļīĆĒĢ£ ĒŖ╣ņØ┤ļÅäĻ░Ć 99%ņśĆļŗż.
ļćīņżäĻĖ░ņŚÉņä£ ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝Ļ│╝ MOGADļŖö ĒśĖļ░£ĒĢśļŖö ļ│æļ│ĆņØś ņ£äņ╣śņŚÉ ņ░©ņØ┤ļź╝ ļ│┤ņØĖļŗż. ņżæļćīņŚÉņä£ļŖö ļæÉ ņ¦łĒÖś ļ¬©ļæÉ ļīĆļćīļŗżļ”¼(cerebral peduncle)ļź╝ ņ╣©ļ▓öĒĢśļéś ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņŚÉ ļ╣äĒĢ┤ MOGADņŚÉņä£ ĻĄÉļćīņØś ņåīļćīļŗżļ”¼(cerebellar peduncle)ņØś ņ╣©ļ▓öņØ┤ ĒØöĒ¢łĻ│Ā(ņśżņ”łļ╣ä, 5.22; 95% ņŗĀļó░ĻĄ¼Ļ░ä, 1.65-16.52), ļō▒ņ¬ĮņŚ░ņłś ņ╣©ļ▓öņØ┤ ļŹö ņĀüņŚłļŗż(ņśżņ”łļ╣ä, 0.20; 95% ņŗĀļó░ĻĄ¼Ļ░ä, 0.09-0.43).22
ĻĖēņä▒ĻĖ░ ņØ┤Ēøä ļ│æļ│Ć Ēü¼ĻĖ░ ļ│ĆĒÖöļÅä ņ¦łļ│æņØä ĻĄ¼ļČäĒĢĀ ņłś ņ׳ļŖö ĒŖ╣ņ¦ĢņØ┤ļŗż. ĒŖ╣Ē׳, MOGADļŖö ļŗżļ░£Ļ▓ĮĒÖöņ”ØņØ┤ļéś ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņŚÉ ļ╣äĒĢ┤ ĻĖēņä▒ĻĖ░ņŚÉ ļ░£ņāØĒĢśļŖö ļćīļ│æļ│ĆņØś ļ®┤ņĀüņØĆ ņāüļīĆņĀüņ£╝ļĪ£ Ēü¼ļéś ĻĖēņä▒ĻĖ░Ļ░Ć ņ¦Ćļé£ Ēøä ļ│æļ│Ć Ēü¼ĻĖ░ņØś Ļ░ÉņåīĻ░Ć ļŹöņÜ▒ ļÜ£ļĀĘĒĢśĻ│Ā, ņÖäņĀä ņåīņŗż(complete resolution)ļÉśļŖö Ļ▓ĮņÜ░ļÅä ļŗżļ░£Ļ▓ĮĒÖöņ”ØĻ│╝ ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņŚÉņä£ļŖö Ļ░üĻ░ü 17%ņÖĆ 10%ņØĖļŹ░ ļ░śĒĢ┤ MOGADņŚÉņä£ļŖö 40%Ļ╣īņ¦Ć ļ│┤Ļ│ĀļÉśņŚłļŗż.23
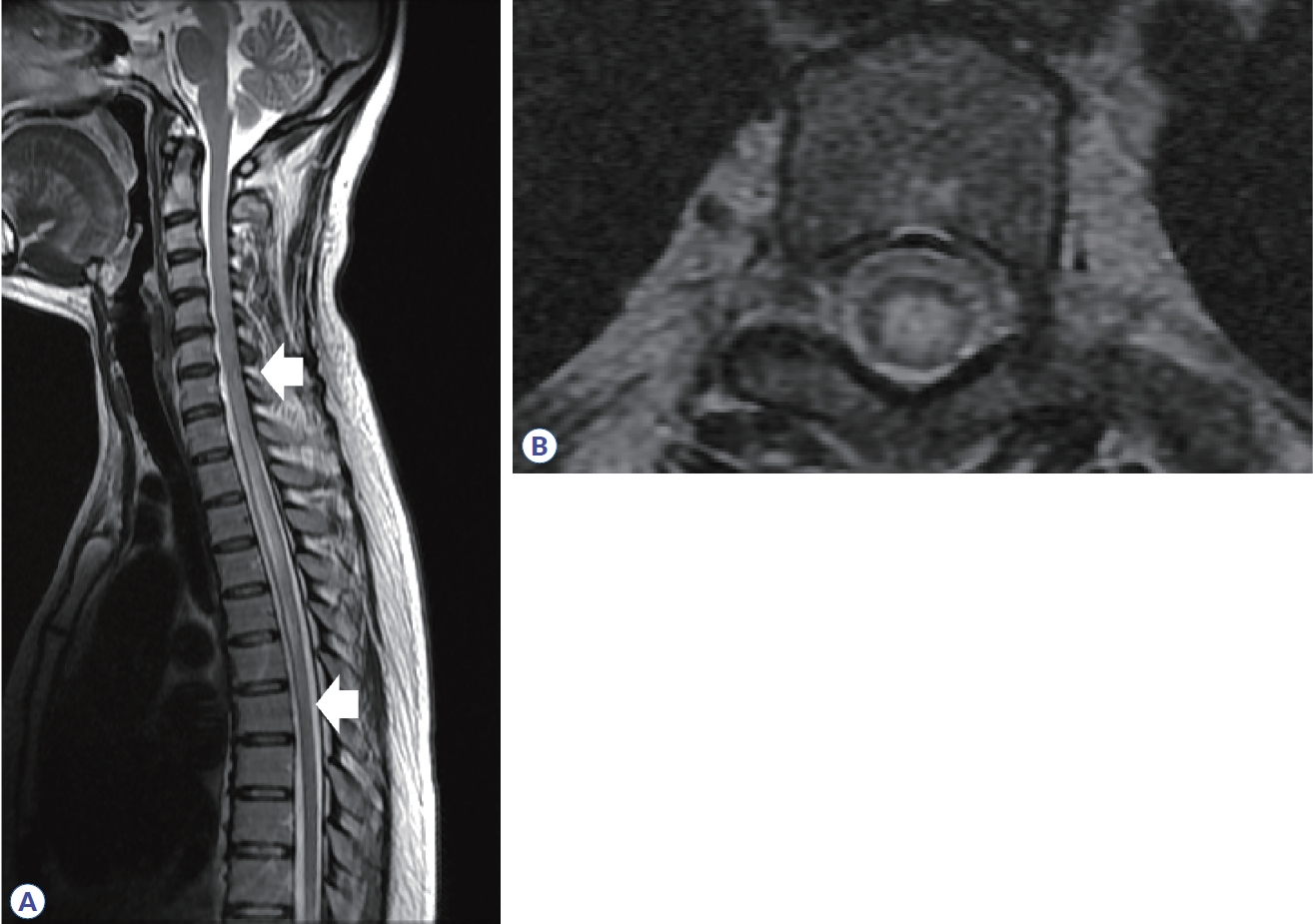
ļŗżļ░£Ļ▓ĮĒÖöņ”Ø, ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝Ļ│╝ MOGADņŚÉņä£ ņ▓ÖņłśņŚ╝ņØś ņśüņāüĒĢÖņĀü ĒŖ╣ņ¦Ģ
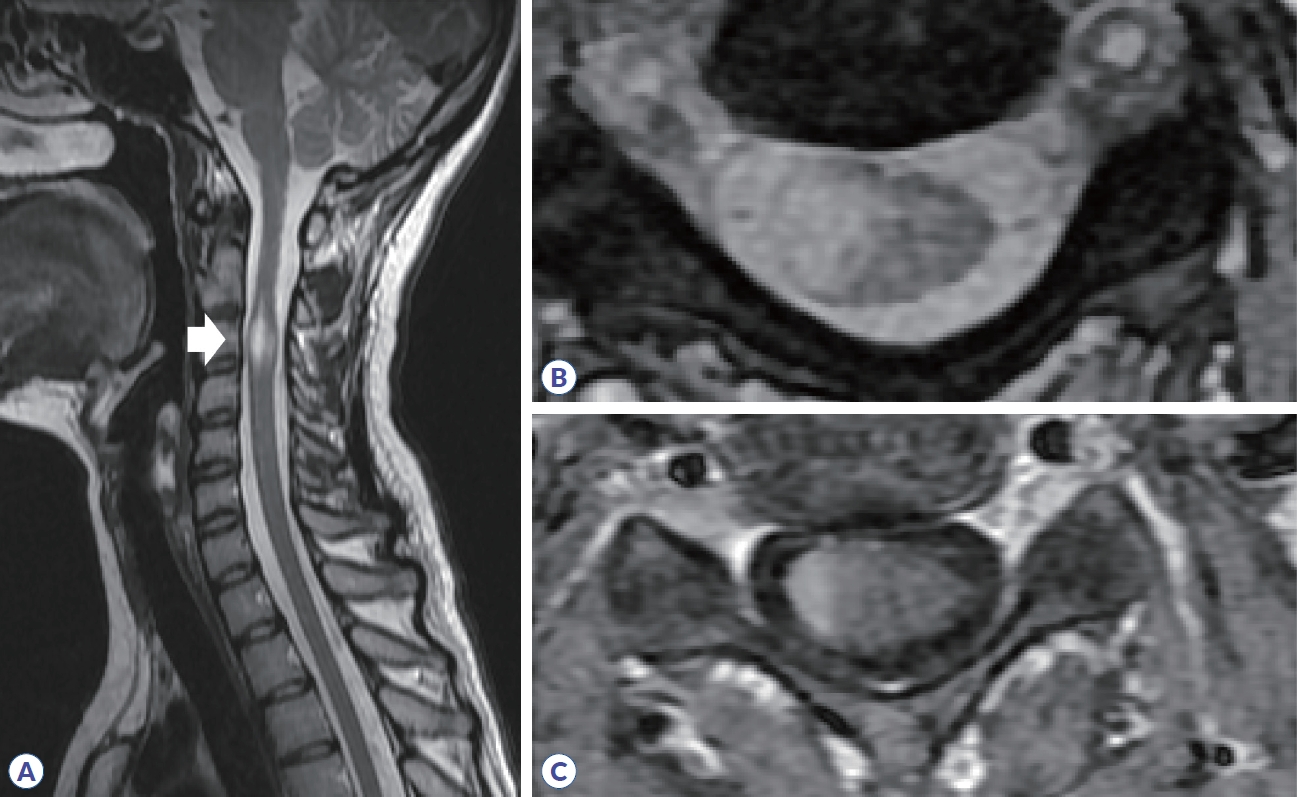
ņ▓ÖņłśņŚ╝ņŚÉ ļīĆĒĢ£ ņøÉņØĖņØä Ļ░Éļ│äĒĢśĻĖ░ ņ£äĒĢ┤ņä£ ļ│æļ│ĆņØś ĻĖĖņØ┤Ļ░Ć ņ▓ÖņČö ļČäņĀł 3Ļ░£ ņØ┤ņāüņØä ņ╣©ļ▓öĒĢśļŖö ņóģļŗ© ļ░®Ē¢źņ£╝ļĪ£ Ļ┤æļ▓öņ£äĒĢśĻ▓ī ņ╣©ļ▓öĒĢśļŖö ĒÜĪļŗ©ņ▓ÖņłśņŚ╝(longitudinally extensive transverse myelitis, LETM)ņØĖņ¦Ć ĒÖĢņØĖĒĢśļŖö Ļ▓āņØ┤ ĒĢäņÜöĒĢśļŗż. ļŗżļ░£Ļ▓ĮĒÖöņ”ØņŚÉņä£ ļ░£ņāØĒĢśļŖö ņ▓ÖņłśņŚ╝ņØĆ ļīĆļČĆļČä ņ¦¦ņØĆ ļ│æļ│ĆņØ┤ļ®░, ņŻ╝ļĪ£ Ļ▓Įņłśļéś ĒØēņłśņŚÉ ĒØöĒĢśĻ│Ā, ņŚ¼ļ¤¼ Ļ░£ņØś ļ│æļ│ĆļōżņØ┤ ņĪ┤ņ×¼ĒĢ£ļŗż(Table 3).24 ļśÉĒĢ£ ņ▓Öņłśļŗ©ļ®┤ņŚÉņä£ ļ│æļ│ĆņØĆ ĒĢ£ņ¬Įņ£╝ļĪ£ ņ╣śņÜ░ņ│ÉņĀĖ(eccentric or wedge shape) ņ׳ļŖö ļČłņÖäņĀä ĒÜĪļŗ©ņ▓ÖņłśņŚ╝(incomplete transvers myelitis)ņ£╝ļĪ£ ļéśĒāĆļé£ļŗż(Fig. 7). ņĪ░ņśüņ”ØĻ░ĢņØĆ ĻĘĀņ¦łĒĢśĻ▓ī ļéśĒāĆļéśĻ▒░ļéś Ļ│Āļ”¼ ņ¢æņāüņØä ļ│┤ņØĖļŗż. ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņØĆ ņĢĮ 85%ņŚÉņä£ LETMņ£╝ļĪ£ ļéśĒāĆļéśļ®░, ļŗ©ņāüņä▒ LETMņØś 50%, ņ×¼ļ░£ņä▒ LETMņØś 93% ņøÉņØĖņØä ņ░©ņ¦ĆĒĢ£ļŗż. Ļ▓Įņłśļéś ĒØēņłśņŚÉ ĒśĖļ░£ĒĢśĻ│Ā, ņĢ×ņä£ ņ¢ĖĻĖēĒĢ£ Ļ▓āņ▓śļ¤╝ ņŚ░ņłśĻ╣īņ¦Ć ļ│æļ│ĆņØ┤ ņØ┤ņ¢┤ņ¦ł ņłś ņ׳ņ£╝ļ®░, ņÖäņĀä ĒÜĪļŗ©ņ▓ÖņłśņŚ╝ņØś ņ¢æņāüņ£╝ļĪ£ ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äļŗż. ĒÜĪļŗ©ļ®┤ ņśüņāüņŚÉņä£ ņ▓ÖņłśņØś ņżæņŗ¼Ļ┤Ć ņŻ╝ļ│Ćņ£╝ļĪ£ ņżæņĢÖļČĆņŚÉ ļ│æļ│ĆņØ┤ ņ£äņ╣śĒĢśļ®░, ņ▓Öņłś ļČĆņóģļÅä ļÅÖļ░śĒĢśļ®░, Ļ│Āļ”¼ Ēś╣ņØĆ ļ░śņĀÉĒśĢ(patchy) ņĪ░ņśüņ”ØĻ░Ģ ņåīĻ▓¼ņØä ņŻ╝ļĪ£ ļ│┤ņØĖļŗż(Fig. 8). ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņŚÉ ņØśĒĢ£ ņ▓ÖņłśņŚ╝ ņżæ ņĢĮ 27-54%ņŚÉņä£ bright/brighter spotty lesionņØ┤ Ļ┤Ćņ░░ļÉśļŖöļŹ░, ĒÜĪļŗ© T2 Ļ░ĢņĪ░ņśüņāüņŚÉņä£ ņ▓ÖņłśņĢĪĻ│╝ ļ╣äņŖĘĒĢśĻ▒░ļéś ļŹö Ļ░ĢĒĢ£ ņŗĀĒśĖļź╝ ļ│┤ņØ┤Ļ│Ā, T1 Ļ░ĢņĪ░ņśüņāüņŚÉņä£ ņ▓ÖņłśņĢĪļ│┤ļŗż Ļ│ĀĻ░ĢļÅä ņŗĀĒśĖļź╝ ļ│┤ņØ┤ļŖö ņåīĻ▓¼ņØä ņØśļ»ĖĒĢ£ļŗż.25,26 ņ×äņāüņĀüņ£╝ļĪ£ Ļ░Ćņ¦ĆļŖö ņØśļ»ĖļŖö ņĢäņ¦ü ļČłļ¬ģĒÖĢĒĢśļéś ļīĆļČĆļČä 2Ļ░£ņøö ņ¦Ćļéśļ®┤ ņåīņŗżļÉśļ®░, MOGADļéś ļŗżļ░£Ļ▓ĮĒÖöņ”Ø, ļŗżļźĖ ņøÉņØĖņØś ņ▓ÖņłśņŚ╝ņŚÉņä£ ņĢĮ 3-6%ļĪ£ ļé«Ļ▓ī ļ│┤Ļ│ĀļÉśņ¢┤ ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņØä ņóĆ ļŹö ņŗ£ņé¼ĒĢśļŖö ņåīĻ▓¼ņØ┤ļØ╝ ĒĢĀ ņłś ņ׳ļŗż. MOGADļŖö LETMņØś 40-80% ņøÉņØĖņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśļ®░, ļ╣ä-LETMņØś ņøÉņØĖņŚÉņä£ 44%ļź╝ ņ░©ņ¦ĆĒĢ£ļŗż.27,28 ļ│æļ│ĆņØ┤ ļŗ©ļ®┤ņĀüņØś 50% ņØ┤ņāüņØä ņ╣©ļ▓öĒĢśļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦ÄĻ│Ā ņŗ£ņāü T2 Ļ░ĢņĪ░ņśüņāüņŚÉņä£ T2 hyperintense lineļĪ£ ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░ņŚÉļŖö ŌĆśpseudodilatation of the central canalŌĆÖņØ┤ļØ╝ ņ¢ĖĻĖēĒĢśĻĖ░ļÅä ĒĢ£ļŗż. ļśÉĒĢ£, ļŗżļ░£Ļ▓ĮĒÖöņ”ØņØ┤ļéś ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņŚÉ ļ╣äĒĢ┤ ņ▓ÖņłśņøÉļ┐ö(conus medullaris)ņØä ņ╣©ļ▓öĒĢśļŖö ļ╣łļÅä(21-41%)Ļ░Ć ļåÆļŗż. ĻĖēņä▒ĻĖ░ņŚÉļŖö ļīĆļČĆļČä ņ▓Öņłś ļČĆņóģņØ┤ ļÅÖļ░śļÉśļ®░ ņĪ░ņśüņ”ØĻ░ĢņØĆ ļ░śņĀÉĒśĢ Ēś╣ņØĆ Ļ▓ĮĻ│äĻ░Ć ļČłļ¬ģĒÖĢĒĢ£ ļ╣äĻĘĀņ¦łĒśĢ ņĪ░ņśüņ”ØĻ░ĢņØä ļ│┤ņØ┤ļéś ļ╣Āļź┤Ļ▓ī ņåīņŗżļÉśĻ▒░ļéś ņĪ░ņśüņ”ØĻ░ĢņØ┤ ņĢł ļÉśļŖö Ļ▓ĮņÜ░ļÅä ņ׳ļŗż. ĒÜĪļŗ©ļ®┤ T2 Ļ░ĢņĪ░ ņśüņāüņŚÉņä£ ĒÜīņāēņ¦łņØä ņ╣©ļ▓öĒĢśņŚ¼ ļéśĒāĆļéśļŖö H-signņØ┤ 29-50%ņŚÉņä£ ļ│┤Ļ│ĀļÉśļ®░, ņØ┤ļŖö ļŗżļ░£Ļ▓ĮĒÖöņ”ØņØ┤ļéś ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝ņŚÉņä£ļŖö 0-8%ļĪ£ ļé«Ļ▓ī ļ│┤Ļ│ĀļÉśņ¢┤ MOGADļź╝ ļŹö ņŗ£ņé¼ĒĢśļŖö ņåīĻ▓¼ņØ┤ ļÉĀ ņłś ņ׳ļŗż. ļćīļ│æļ│ĆĻ│╝ ļ¦łņ░¼Ļ░Ćņ¦ĆļĪ£ ļ│æļ│ĆņØś ņÖäņĀä ņåīņŗżņØ┤ 62-79%ļĪ£ ļåÆņ£╝ļ®░ ļ│æļ│Ć ļČĆņ£äņØś ņ▓Öņłś ņ£äņČĢņØĆ 3-10%ļĪ£ ļō£ļ¼╝Ļ▓ī ļ░£ņāØĒĢ£ļŗż.23,29
ĻĖ░ĒāĆ ņżæņČöņä▒ ņŚ╝ņ”Øņ¦łĒÖśņØś ņśüņāüĒĢÖņĀü ĒŖ╣ņ¦Ģ
ADEMņØĆ ņŻ╝ļĪ£ ņåīņĢäņŚÉņä£ ĒØöĒ׳ ļ░£ņāØĒĢśļ®░, ņĢĮ 3/4ņŚÉņä£ ņäĀĒ¢ē ļ░öņØ┤ļ¤¼ņŖż Ļ░ÉņŚ╝ņØä ļÅÖļ░śĒĢ£ļŗż.2 ļīĆļČĆļČä ņ×äņāüņĀüņ£╝ļĪ£ ļŗ©ņāüņä▒ Ļ▓ĮĻ│╝ļź╝ ļ│┤ņØ┤ļéś ņØ╝ļČĆņŚÉņä£ļŖö ņ×¼ļ░£ĒĢśļŖö Ļ▓ĮĻ│╝ļÅä ļ│┤Ļ│ĀļÉ£ļŗż. ļ│æļ│ĆņØĆ ņŗ£ņŗĀĻ▓Į, ļćī, ņ▓Öņłś ļ¬©ļæÉ ļ░£ņāØņØ┤ Ļ░ĆļŖźĒĢśļ®░, ļćī ņ×ÉĻĖ░Ļ│Ąļ¬ģņśüņāüņŚÉņä£ļŖö 1 cm ņØ┤ņāü, ļ»Ėļ¦īņä▒ņØś Ļ▓ĮĻ│äĻ░Ć ļČłļČäļ¬ģĒĢ£(ŌĆśfluffyŌĆÖ) ļ│æļ│ĆļōżņØ┤ ņŻ╝ļĪ£ ļ░▒ņ¦łņØä ņ╣©ļ▓öĒĢśļŖö ņ¢æņāüņØ┤Ļ│Ā, ņŗ£ņāü ļō▒ Ļ╣ŖņØĆ ĒÜīņāēņ¦ł ļ│æļ│ĆļÅä ļÅÖļ░śļÉĀ ņłś ņ׳ļŗż.
ĻĘĖ ņÖĖ ļŗżņ¢æĒĢ£ ņŚ╝ņ”Øņ¦łĒÖśļ│äļĪ£ ļćīņŗżņ¦łņŚÉņä£ ĒśĖļ░£ĒĢśļŖö ļ│æļ│Ć ņ£äņ╣śĻ░Ć ņĢīļĀżņĀĖ ņ׳ļŗż. ļ│ĆņŚŁĻ│äņŚÉ ļ│æļ│ĆņØ┤ ļ░£ņāØĒĢśļŖö Ļ▓ĮņÜ░ ņ×ÉĻ░Ćļ®┤ņŚŁļćīņŚ╝ņØ┤ļéś ĒĢśņŗ£ļ¬©ĒåĀļćīļ│æņ”ØņŚÉ ļīĆĒĢ£ Ļ│ĀļĀżĻ░Ć ĒĢäņÜöĒĢśĻ│Ā ĒŚżļź┤ĒÄśņŖżļćīņŚ╝Ļ│╝ Ļ░Éļ│äņØä ĒĢ┤ņĢ╝ ĒĢ£ļŗż. ļ®┤ņŚŁĻ┤Ćļ¼Ė ņ¢ĄņĀ£ņĀ£ļź╝ Ēł¼ņŚ¼ļ░øļŖö ĒÖśņ×ÉņŚÉņä£ļŖö ļŗżļ░£ņä▒ Ēö╝ņ¦łĒĢś ļ│æļ│ĆņØ┤ ļ░£ņāØĒĢĀ ņłś ņ׳ļŗż. Ļ╣ŖņØĆ ĒÜīņāēņ¦łņØä ņ╣©ļ▓öĒĢĀ ņłś ņ׳ļŖö ņ¦łĒÖś ņżæ ĒĢŁCRMP5/CV2ļćīņŚ╝ņØ┤ļéś ĒĢŁDR2ļćīņŚ╝ņØĆ ņżäļ¼┤ļŖ¼ņ▓┤ļź╝ ņל ņ╣©ļ▓öĒĢśĻ│Ā, ĒĢŁMa2ņŚ░Ļ┤Ć ļćīņŚ╝ņØś 74%ņŚÉņä£ļŖö ņé¼ņØ┤ļćī ņ╣©ļ▓öņØ┤ ļéśĒāĆļé£ļŗż. ļ▓Āņ▓┤ĒŖĖļ│æņØ┤ļéś ņé¼ļź┤ņĮöņØ┤ļō£ņ”Ø, chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroidsļŖö ļŖźĒśĢļćīņŚ╝(rhombencephalitis)ņØä ņל ņØ╝ņ£╝ĒéżļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż.30 ņŗĀĻ▓ĮĻĄÉņä¼ņ£Āņ¦ł ņé░ņä▒ ļŗ©ļ░▒ņ¦ł ņłśļ¦ēļćīņŚ╝(glial fibrillary acidic protein meningoencephalitis, GFAP meningoencephalitis)ņØĆ ļćīņŗż ņŻ╝ļ│Ćņ£╝ļĪ£ ļ░®ņé¼ņäĀĒśĢ(radial linear) ņĪ░ņśüņ”ØĻ░ĢņØä ļ│┤ņØ┤ļŖö Ļ▓āņØ┤ ĒŖ╣ņ¦ĢņĀüņØ┤ļŗż.31 ņØ╝ļČĆ ņżæņČöņŗĀĻ▓ĮĻ│ä ņŚ╝ņ”Øņä▒ ņ¦łĒÖśņŚÉņä£ļŖö ļćīņłśļ¦ē ņĪ░ņśüņ”ØĻ░ĢņØ┤ ļō£ļ¼╝ņ¦Ć ņĢŖĻ▓ī ļÅÖļ░śļÉ£ļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ļŗż.2 ņé¼ļź┤ņĮöņØ┤ļō£ņ”ØņØś ņĢĮ 49%ņŚÉņä£ ņŚ░ņłśļ¦ē, 32%ņŚÉņä£ Ļ▓Įņłśļ¦ē ņĪ░ņśüņ”ØĻ░ĢņØä ļ│┤ņØ┤ļŖöļŹ░, ļćīņłśļ¦ē ņĀäņ▓┤ņŚÉ Ļ▒Ėņ│Éņä£ ņĪ░ņśüņ”ØĻ░ĢņØ┤ ļéśĒāĆļéśĻ▒░ļéś Ļ▓░ņĀłņä▒ ļ¬©ņ¢æņØä ļ│┤ņØ╝ ņłś ņ׳Ļ│Ā, ļ│æļ│Ć ņ£äņ╣śņŚÉ ļö░ļØ╝ ĒÅÉņćäņä▒ ņłśļæÉņ”ØņØ┤ ļÅÖļ░śļÉśĻĖ░ļÅä ĒĢ£ļŗż. ļźśļ¦łĒŗ░ņŖżĻ┤ĆņĀłņŚ╝ļéś ņ£ĪņĢäņóģņ”Ø ļŗżļ░£ĒśłĻ┤ĆņŚ╝ņØ┤ ņżæņČöņŗĀĻ▓ĮĻ│äļź╝ ņ╣©ļ▓öĒĢśļŖö Ļ▓ĮņÜ░ļÅä ļćīņłśļ¦ē ņĪ░ņśüņ”ØĻ░ĢņØ┤ ļéśĒāĆļéĀ ņłś ņ׳ņ£╝ļ®░, ļ®┤ņŚŁĻĖĆļĪ£ļČłļ”░ G4 Ļ┤ĆļĀ© ņ¦łĒÖśņØĆ Ļ▓Įņłśļ¦ēņŚ╝ņØ┤ Ļ░Ćņן ĒØöĒĢ£ ņżæņČöņŗĀĻ▓ĮĻ│ä ņ╣©ļ▓ö ņ¢æņāüņ£╝ļĪ£ ļćīĒĢśņłśņ▓┤ņŚ╝ņØ┤ļéś ĒĢ┤ļ®┤ņĀĢļ¦źļÅÖ ņØ┤ņāü ņåīĻ▓¼ņØä ļ│┤ņØ╝ ņłśļÅä ņ׳ļŗż.
ņ▓Öņłśļź╝ ņ╣©ļ▓öĒĢśļŖö Ļ▓ĮņÜ░, ļČĆņóģņ¢æņ×ÉĻ░Ćļ®┤ņŚŁņ▓ÖņłśņŚ╝ņØĆ ņŗĀĻ▓ĮļĪ£ĒŖ╣ņØ┤(track-specific) ļ│æļ│ĆņØä ļ│┤ņØ┤Ļ│Ā, ņé¼ļź┤ņĮöņØ┤ļō£ņ”ØņØĆ ļ░░ņ¬Į Ēś╣ņØĆ ļō▒ņ¬Į ņŚ░ņ¦łļ¦ēĒĢś ņĪ░ņśüņ”ØĻ░ĢņØ┤ ļ│┤ņŚ¼ ŌĆśbraidŌĆÖ Ēś╣ņØĆ ŌĆśtridentŌĆÖ ņ¢æņāüņØ┤ Ļ┤Ćņ░░ļÉ£ļŗż. ļ▓Āņ▓┤ĒŖĖļ│æņØś ņ▓Öņłś ļ│æļ│ĆņŚÉņä£ļŖö ļ│æļ│Ć ņŻ╝ļ│ĆļČĆ(rim) ņĪ░ņśüņ”ØĻ░ĢņØ┤ Ļ┤Ćņ░░ļÉśļŖöļŹ░, ĒÜĪļŗ©ļ®┤ ņśüņāüņŚÉņä£ ŌĆśbagel signŌĆÖņ£╝ļĪ£ ļ│┤ņØ╝ ņłś ņ׳ļŗż.32 ļćīļ│æļ│ĆĻ│╝ ņ£Āņé¼ĒĢśĻ▓ī ļ░®ņé¼ņäĀĒśĢ ņĪ░ņśüņ”ØĻ░ĢņØ┤ ļéśĒāĆļéśļŖö Ļ▓ĮņÜ░ GFAPņ▓Öņłśļ│æņØä Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢ£ļŗż.31
Ļ▓░ļĪĀ
ņśüņāüĒĢÖņĀü ņåīĻ▓¼ņØĆ ņżæņČöņŗĀĻ▓ĮĻ│ä ņŚ╝ņ”Øņä▒ ņ¦łĒÖśļōżņØä Ļ░Éļ│äĒĢśļŖö ļŹ░ ņżæņÜöĒĢ£ ļŗ©ņä£ļź╝ ņĀ£ņŗ£ĒĢ£ļŗż. Ļ░ü ņ¦łĒÖśņŚÉ ļö░ļźĖ ņĀäĒśĢņĀüņØĖ ņśüņāüĒĢÖņĀü ņåīĻ▓¼ņØä ņłÖņ¦ĆĒĢśļŖö Ļ▓āņØ┤ ĒĢäņÜöĒĢśļ®░, ļ│æļ│ĆņØś ļ¬©ņ¢æĻ│╝ ņ£äņ╣ś, ĻĖĖņØ┤, ņĪ░ņśüņ”ØĻ░Ģ Ēī©Ēä┤Ļ│╝ ĻĖēņä▒ĻĖ░Ļ░Ć ņ¦Ćļé£ Ēøä ļ│æļ│ĆņØś ĒÜīļ│Ą ļ░Å ņ£äņČĢ ļō▒ņØä ņŻ╝ņØś Ļ╣ŖĻ▓ī ņé┤ĒÄ┤ļ│┤ņĢäņĢ╝ ĒĢ£ļŗż. ļśÉĒĢ£, Ļ│ĀņŗØņĀü ņ×ÉĻĖ░Ļ│Ąļ¬ģņśüņāü ņØ┤ņÖĖņŚÉļÅä OCTļéś ĒŖ╣ņłśĻĖ░ļ▓Ģņ£╝ļĪ£ ņ┤¼ņśüĒĢ£ ņśüņāüņØä ņØ┤ņÜ®ĒĢśņŚ¼ Ļ░Éļ│äņŚÉ ĒĢäņÜöĒĢ£ ņĀĢļ│┤ļź╝ ņ¢╗ņØä ņłś ņ׳ļŗż. ļŗżļ░£Ļ▓ĮĒÖöņ”Ø, ņŗ£ņŗĀĻ▓Įņ▓ÖņłśņŚ╝, MOGAD ņÖĖņŚÉļÅä ņ×ÉĻ░Ćļ®┤ņŚŁļćīņŚ╝ņØ┤ļéś ļźśļ¦łĒŗ░ņŖżņ¦łĒÖś ļō▒ ļŗżņ¢æĒĢ£ ņ¦łĒÖśļōżņØ┤ ņżæņČöņŗĀĻ▓ĮĻ│ä ņŚ╝ņ”Øņä▒ ņ¦łĒÖśņØä ņ£Āļ░£ņŗ£Ēé¼ ņłś ņ׳ņ£╝ļ»ĆļĪ£ ĒĢŁņāü Ļ░Éļ│ä ņ¦äļŗ©ņ£╝ļĪ£ ņŚ╝ļæÉņŚÉ ļæÉļŖö Ļ▓āņØ┤ ĒĢäņÜöĒĢśĻ▓Āļŗż.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



